|
Background | Study Design | Treatment | Results | Comments
Peng B, Wenwen W, et al. “Chemical Radiculitis." (2007) Pain 127(11-16)
Background:
In 1997 Marshall et al. [1] was the first to put forth the idea that a torn annulus fibrosis (annulus), without physical nerve root compression, could result in debilitating low back pain, as well as radiating lower extremity pain (sciatica, radiculopathy, radiculitis). The cause of the sciatica was believed to be secondary to the irritation of the adjacent nerve roots from the leakage of biochemicals from the disc. Hence, the theory of chemical radiculitis was born. This theory has intrigued many a spinal surgeon for years, but to date the syndrome remains mysterious.
Throughout the late 1980s and 1990s, researchers have worked to elucidate the phenomenon of chemical radiculitis. More specifically, in 1987, McCarron et al. published the results of a small investigation where they harvested autologous nucleus pulposus (nucleus pulposus from the dog's own disc) from a small cohort of dogs and then transferred it upon the surgically-exposed thecal sac/nerve roots. After three weeks the animals were destroyed and microscopic examination of the exposure site ensued. In all of the experimental dogs, the thecal sac and nerve roots demonstrated evidence of inflammation; however, none of the control group had such signs.
In 1993, Olmarker et al. [2] carried the experimentation a step further when they placed porcine (pig) autologous nucleus pulposus in the epidural space upon the thecal sac. There experimental procedure ensured there is no physical compression upon the thecal sac (a criticism of the previous work). A control group was set up where retroperitoneal fat was used instead of nucleus pulposus. The animals were killed and the nerve roots were carefully examined histologically. Nerve fiber injury was discovered in all of the experimental animals, but the control animals had no such injury.
Study Design:
In this Chinese investigation, 42 patients with chronic low back pain and strong lower extremity pain were recruited for study. Inclusion criteria included leg pain greater than low back pain and imaging studies that were negative disc herniation or bulging (i.e., MRI and CAT scan were completely normal looking). Furthermore, all of these patients were discogram positive for concordant pain and all of them demonstrated annular disruption at a single level. They had also failed all attempts at conservative care including physical therapy and nonsteroidal anti-inflammatory medication. EMG/NCV testing was also performed before the treatment and all patients completed a preoperative visual analog pain scale, as well as the Oswestry disability test.
Perhaps surprisingly, 32 patients (76%) demonstrated EMG findings that included abnormal insertional activities such as fibrillation potentials, positive sharp waves, and/or polyphasic motor unit potentials (MUPs), notwithstanding the appearance of a compressive disc herniation on imaging.
The average postsurgical follow-up period for these patients was 2.7 years (one – five years). All of them were available for follow-up.
The Treatment:
All patients were treated with surgical intervention that included anterior lumbar interbody fusion (ALIF) posterior lumbar interbody fusion (PLIF), and prosthetic nucleus pulposus displacement (PDN).
Statistics:
Student’s t-tests were used to determine whether the average difference between scores before and after surgery were statistically significant. Chi-square criterion and Spearman correlation test were also used.
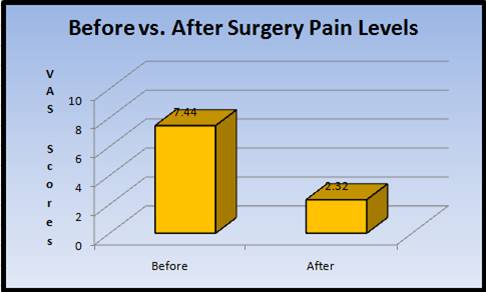
Results:[VAS | ODI ]
Of the 42 patients, "One showed no evidence improvement, and another one still complained of low back pain and weakness in both lower extremities." That is, there was a 4.8% failure rate with the fusion surgeries. The rest of the patients (95%) ostensibly reported complete relief or marked improvement with regard to their low back pain and lower extremity pain.
With regard to VAS, the median score was reduced from 7.74 to 2.32, with a mean reduction of 5.12 (p = 0.000).
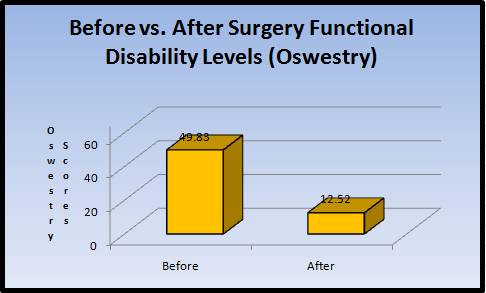
With regard to the Oswestry scores (see below), a median improvement of 76% was recorded (49.83 to 12.52, p=0001).
One interesting discography result: the patients with unilateral posterolateral annular disc disruptions mainly presented with unilateral lower extremity pain. However, in the patients who suffered annular tears on both posterolateral aspects of the disc or who suffered a central annular tear, there complaints were bilateral lower limb pain (chi-square criterion, X2 = 14.92, df=3, p=0.0019).
Comments:
I Don't believe I have ever seen a study on lumbar interbody fusion with such high outcome results--it a little unbelievable. However, the reason I publish this review is to draw attention to the phenomenon of discogenic pain. Just because your MRI does not show a disc herniation does not mean that there is nothing wrong with the disc. In these patients, all of there MRIs were normal, yet they suffered terrible, debilitating pain in the lower back, as well as down the leg which ultimately led to fusion. So it does exist, and if your doctor is not familiar with it, the medical literature is right with information about it.
References:
1) McCarron RF et al. “The inflammatory effect of nucleus pulposus. A possible element in the pathogenesis of low back pain." Spine 1987; 12(8): 760-4.
2) Olmarker K, et al. “Autologous Nucleus pulposus induces neurophysiologic and histologic changes in porcine cauda equina nerve roots.” Spine 1993; 18(11):1425-32.
Top
© Copyright 2002 – 2012 by Dr. Douglas M. Gillard DC - All rights reserved
|
