Herzog R, et al. "Variability in diagnostic error rates in 10 MRI centers performing lumbar spine MRI examinations on the same patient within the three-week period." Spine J 2017; 17:554 –561.
Early in 2017, Hospital for Special Surgery’s, Dr. Richard Herzog, et al., published the results of fascinating study in one of the top Spine Journals in the world, The Spine Journal. Basically, in this first-of-its-kind study, the researchers sent a single chronic low back patient to 10 different MRI centers for a MRI scan, within a very short period of time. Then all the radiology reports were gathered and compared for accuracy and uniformity. Although you would expect that all of these reports would would be similar, that was not the case at all!
Here’s the details: a 63-year-old female, who suffered chronic back and classic radicular pain, underwent magnetic resonance imaging scanning (i.e., had an MRI) at the study’s testing center. Her images were then reviewed by two veteran, board certified radiologists who are specially trained and certified in imaging of the spine. You can consider them as “super-radiologists,” who do not make mistakes when it comes to reading images of the spine. After finishing their analysis of the MRI images, both radiologists independently agreed that the patient had three very common chronic-pain-causing spinal conditions: disc herniation, spondylolisthesis, and severe spinal stenosis. Furthermore, all of these conditions were associated with significant nerve root compression. {There were other more subtle and more complicated MRI findings gleaned by these super radiologists, but I will leave these out of this review in attempts to keep it as simple as possible. However, you should know that the other radiologists screwed up these findings just as badly as they did the big three above!}
Over the next three weeks, this same patient randomly presented to 10 different MRI centers throughout the Greater New York area for the purpose of getting a new MRI and a new radiology report from each one. None of these MRI centers, which were all certified by the American College of radiology, or their radiologists had any idea that the patient was part of this study. At each center, she gave the same history of injury and other intake information, but she did not reveal that she had previously had MRIs, or that she was part of the study – that was top-secret!
Finally, after the 10 random MRIs/radiology reports had been obtained, she underwent one more MRI back at the original MRI testing center, just to make sure her condition had not changed over that previous three-week period, which it didn’t.
The 10 MRI reports from those random MRI center visits were next compared to the true MRI findings and the shocking results were published.
 First the good news: nine out of 10 radiologists (90%) correctly describe the spondylolisthesis that was present. Remember, spondylolisthesis (figure left) is so easy to see that a first-year chiropractors/medical doctor could easily spot it. Pretty sad that one radiologist completely missed it! The overwhelming majority of the radiologists, however, screwed up the associated nerve root compression. (See below) First the good news: nine out of 10 radiologists (90%) correctly describe the spondylolisthesis that was present. Remember, spondylolisthesis (figure left) is so easy to see that a first-year chiropractors/medical doctor could easily spot it. Pretty sad that one radiologist completely missed it! The overwhelming majority of the radiologists, however, screwed up the associated nerve root compression. (See below)
[Figure left demonstrates a sagittal {from the side} view of a run-of-the-mill spondylolisthesis of L4 on L5. Note the forward slip. Pretty hard to miss this, right? [Note: note: I have used an image for my collection and have not violated the Copyright protection afforded by the Journal.]
Now the bad news: With regard to correctly making the diagnosis for the central spinal stenosis, the “miss-rate (i.e., they screw-up the diagnosis)” was a whopping 45%! In other words, only 55% of the radiologists properly caught and described the central spinal stenosis.
With regard to disc herniation, the miss-rate was 47.5%!
The miss-rate for catching and properly describing the nerve root compression, caused by either disc herniation, spondylolisthesis and central stenosis, was a whopping 72.5%!
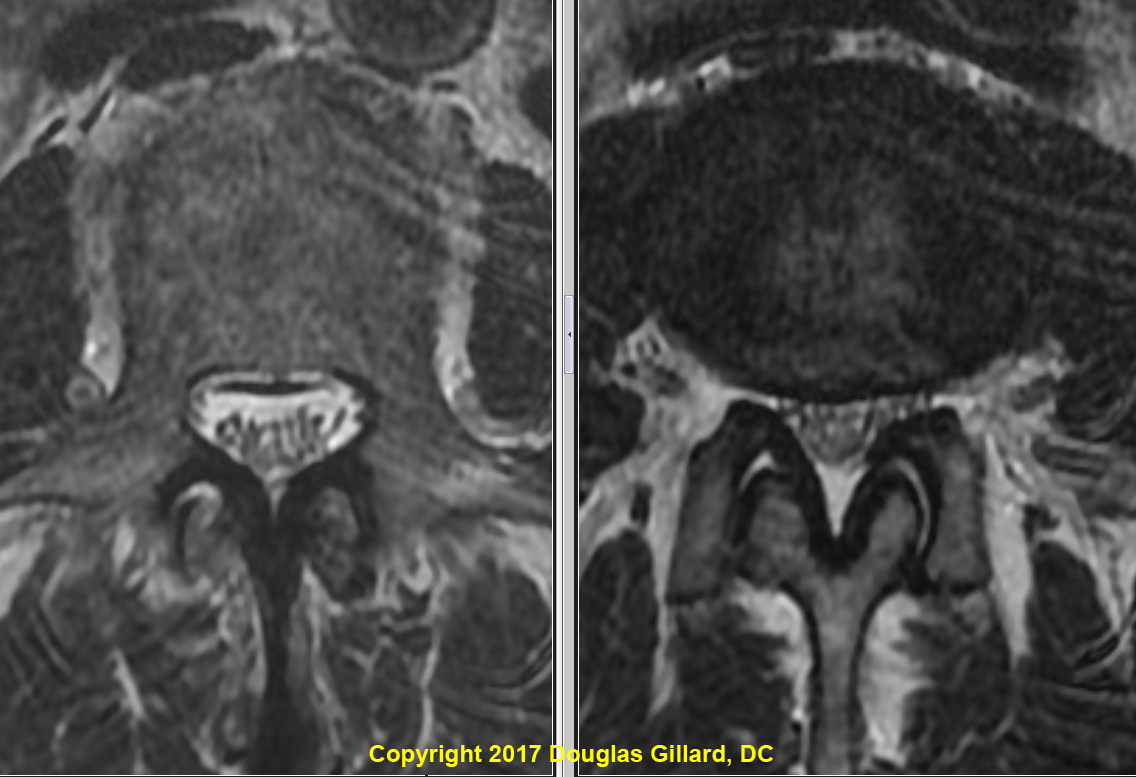
Let’s take a more specific example. The patient had severe central stenosis at L2/3, which look like the below picture. (Note: again, I don’t want to violate the Journal’s Copyright protection on this paper/images, so I’ve used images from my own collection that look almost exactly like the images used in the paper. If anything, the image used in the paper demonstrated an even more dramatic difference which really shouldn’t have been missed by anybody! I would speculate that 80% of my eighth quarter chiropractic students would've caught this!)
The image on the below-left shows a normal thecal sac which is not deformed or compressed (always use the image at the pedicle level above the disc that is stenotic). You can see all the nerve roots floating around (black dots) in the cerebral spinal fluid (bright white stuff), happy as can be. {If you’re having trouble seeing this, please study my anatomy page, MRI page and/or stenosis page in order to get up to speed.}
The image on the below-right, however, demonstrates a thecal sac that has lost a significant amount of its volume (a 66% loss or more is the definition for severe stenosis) because it’s getting “squished” by ligamentum flavum thickening and a bulging disc. There’s no question that it is significantly smaller than the thecal sac on the left. In fact, the nerve roots of the cauda equina are so squished, that you can’t see any white cerebrospinal fluid around them. This example represents moderate-severe spinal stenosis.
How did the New York radiologists do with regard to identifying this obvious severe stenosis? Shockingly, 40% of them completely missed it! That's right, they didn't even see it! That is completely un-excusable! Of the 60% of radiologists who actually saw it, only one of them actually described it correctly! In other words, only 10% saw it and described it correctly! Again, completely ridiculous.
DISCUSSION:
Who cares about this? Except for spine surgeons and other spine specialists who read their own MRIs, chiropractors, physical therapists, general practitioners, and family docs all typically heavily rely on that radiology report to make their diagnosis, order additional testing and prescribed treatment. Furthermore, insurance claims adjusters and attorneys also rely on these radiology reports to authorize treatment and fight for settlements, respectively.
So what? Well, as confirmed by the authors, these inaccurate reports may well lead to misdiagnosis; inappropriate treatment and/or lack of treatment; delayed treatment authorization; underpayment or overpayment in court settlements; and, perhaps most importantly, poor clinical outcomes. For example, we know that the timing for discectomy surgery is crucial for the achievement of a good clinical outcome. If a radiologist misses a compressive disc herniation, this will most likely cause a significant delay in the surgery which in turn, according to research, may significantly decrease the chance for a good clinical outcome. Shouldn’t the radiology center and radiologist be held liable for such a blatant miss, just like they would if they missed a cancer? I absolutely think so.
Anecdotally, I have known for years that many radiologists are really bad at picking out and adequately describing the typical pain generators that may be responsible for the patient’s pain syndrome. Although they are typically very good at picking out things that will kill the patient (fracture, infection, hemorrhage, metastatic disease, etc.) and potentially get them and their clinics sued. In fact, this phenomenon was the impetus for the development of my coaching service.
The $64,000 question is why are radiologists doing such a terrible job at reading the MRI images and then generating a good report? I have some theories:
Reading time: I know several radiologists personally and based on my conversations with them, there is one huge problem: they are not given enough time by the MRI center to properly go through these images! For example, one radiologist I know who works for a prominent MRI center stated that they are only allowed eight minutes per patient! Eight minutes per patient!! That’s absolutely ridiculous, especially on cases that have multiple findings, like the one in the study.
Laziness/burnout: radiologists have to read off a lot of images each day. Therefore, it’s possible that they are just getting burned out and don’t put much effort forth, other than making sure the patient doesn’t have any serious disease. This sort of relates to the reading time problem.
Brainpower?: anecdotally it is known that the smartest medical students “typically” go after and get the more sought after specialties, like neurosurgery. The students who don’t do as well on the USMLE examinations and other testing are typically forced into the subspecialties that most doctors don’t want to go into, one of which is radiology and another is psychiatry. Therefore, perhaps, some of these radiologists don’t have the skill to pick out subtle pain generators other than the obvious spondylolisthesis (although one radiologist even missed that!).
Final Comments: although this is a very small study and needs to be repeated on a much larger scale, I hope that the results of this paper, which are a real slap in the face to the American College of radiology, will be the impetus for change within the radiology industry. Perhaps, akin to the work-hour-limitations placed on truck drivers and airline pilots, limitations should be placed on radiologists with regard to how many scans they are allowed to read in an eight hour day. I would speculate that there are many patients out there with now-chronic pain syndromes which occurred as a direct result of a radiology report which missed a key diagnosis.
Copyright 2017 Douglas Gillard, DC
|
