
Epidural Steroid Injections
General Information | Fluoroscopically Guidance | The Three Types of ESI | Bottom Line
Epidural Steroid Injections: General Information
Treated Conditions | How Does It Work? | Does It Work? | Risks | ESI vs. Selective Nerve Root Block
 An epidural steroid injection (ESI) is a moderately invasive procedure that may be ordered by a doctor if conservative care (physical therapy, chiropractic care, acupuncture, and medication) has failed to relieve complaints of lower limb and/or low back pain.
An epidural steroid injection (ESI) is a moderately invasive procedure that may be ordered by a doctor if conservative care (physical therapy, chiropractic care, acupuncture, and medication) has failed to relieve complaints of lower limb and/or low back pain.
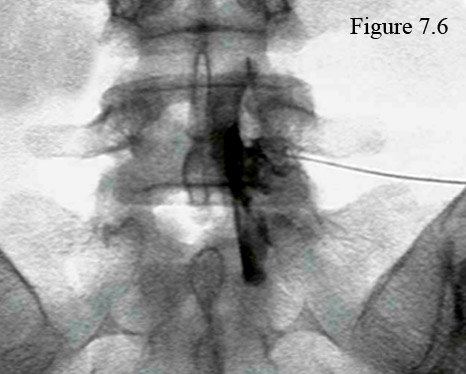
Figure 7.6 is an anterior-posterior fluoroscopic image that was taken during an epidural steroid procedure that was done for a symptomatic L5/S1 disc herniation. Note the nearly horizontal positioned needle on the right that has just injected contrast and a steroid (black) into the neuroforamen and spinal canal in attempts to cover an L5/S1 disc herniation and the traversing S1 nerve root. Can't see what I'm talking about? Click here for some help.
Epidural steroid injections are for the treatment of lower limb pain (aka: radicular pain, sciatica, or radiculopathy) that is caused by compression and inflammation of either the traversing or exiting nerve root. (*If I just lost you, then please visit my Disc Anatomy Page and then the Disc Herniation Page in order to get up to speed on terminology.) Such compression and inflammation is typically the result of the disc herniation and/or lateral stenosis.
In addition to the treatment of sciatica, ESIs have also been found efficacious (safe and effective) for the treatment of disc-herniation-related or annular-tear-related lower back pain. [1-6] However, these injections are typically not very effective for the treatment of central stenosis, scoliosis (unless there is foraminal collapse), spondylolisthesis, spondylolysis, facet syndrome, or sacroiliac syndrome.
ESI: what is it, and how does it work?
In a nutshell, the ESI procedure, which has been around since the 1950s, involves the careful insertion of a thin needle into the posterior or anterolateral epidural space at the level of the disc herniation, annular tear or lateral stenosis.
After the needle is confirmed to be in the proper position, then 1.5-10mL a corticosteroid (a very powerful anti-inflammatory) and anesthetic are injected into the area. The steroid will bathe the inflamed tissue in hopes of reducing the pain-causing inflammation, and the anesthetic will not only numb the inflamed structures, it will also wash away any pro-inflamatory biochemicals (cytokines for the most part) that happen to be in the area.
Over the past decade, the popularity of ESIs have greatly increased. Specifically, Manchitanti et al. reported that, [13] after studying Medicare data, the general utilization of all ESI procedures has increased between 2000 and 2011 by over 130%, and the use of lumbar transforaminal epidural steroid injections (TFESIs) has skyrocketed by over 600%! [13] *We shall discuss the three different ESI techniques farther below.
Does the ESI have to be repeated?
The short answer is yes, anecdotally ESIs do have to be repeated in order to get a good effect. Although there is no solid research to support the common practice of using a series of two or three epidural steroid injections, [14] typically patients are asked to return for second and then third procedure every six months or so. [3] However, if the first ESI fails to provide any pain relief, then the chance of a second or third procedure working are very low and probably not worth the risk, cost, and inconvenience.[10]
Who should perform the ESI procedure?
Although physicians of many different specialties are doing this procedure in this day and age of post-Obama care, only a fellowship-trained interventional pain medicine physician—one who has devoted his entire practice to performing these injective procedures—would be good enough to treat my patients or me. [3]
Do ESIs really work?
There has been a lot of quality research performed on ESIs, and the short answer is yes, they do work. However, the medical literature has indicated that their effectiveness is usually limited to less than six months. In other words, the pain typically returns within six months; however, anecdotally, that pain is usually of a lesser intensity. [2,7]
It is also important to note that if you have waited longer than one year to try ESIs, or if you have spondylolisthesis, then the chances of obtaining a successful outcome from the injections are not very good. [7]
What are the risks of having an ESI?
Just like any surgical procedure, there are health risks associated with undergoing an ESI. Specifically, complications from inadequate sterilization, poor needle placement, or the accidental injection of the injectate (i.e., the steroid and anesthetic) into either a vein or artery include severe infection (0.1-0.01%), hematoma (7X10^-6% {Avery, very small chance}), nerve root trauma, intravascular injection (11.2% w/ TFESI and 1.9% with ILESI), dural sac puncture, and air embolism. [11]
Just like with oral corticosteroids, ESIs may also increase the chance of developing osteoporosis, especially in the vertebral body, and made lead to vertebral body fracture in rare cases.
What is the difference between an ESI and a Selective Nerve Root Block?
Here is one of the most common questions I get in my e-mail inbox: what is the difference between and ESI and a selective nerve root block (SNRB)?
An ESI is a therapeutic procedure that has the objective of long-term reduction of back and leg pain. Therefore, although it may use an anesthetic such as lidocaine, its main payload (injectate) is that of a cortical steroid, which is more likely to accomplish long-term pain relief than lidocaine alone.
A SNRB, on the other hand, is a diagnostic procedure that has the objective of very short term pain relief. Therefore, its payload is only an anesthetic or a combination of anesthetics, such as Lidocaine (very short-term anesthetic) and Marcaine (slightly longer-term anesthetic), which can be delivered in a low-volume and thereby eliminate any volume reaction (a flareup of pain from a larger volume of injectate physically irritating and inflamed nerve root).
That's all the deeper I'm going to go with regard to SNRBs, but I would be more than happy to discuss this further with you on the phone during one of my Coaching Sessions. (learn more)
What is the bottom line?
The bottom line seems to be that ESIs are relatively safe and effective for treating severe flareups of back and/or leg pain. However, they are probably not going to have any influence on the long-term outcome of your condition. In other words, in the long run, it probably won't make difference whether or not you have had them.
Okay, it's time to go a little deeper.
Epidural Steroid Injection: Fluoroscopic Guidance
Another very important component of the ESI procedure is fluoroscopic imaging, which should always be used in order to ensure correct needle placement and avoid the common complication of intravascular injection; i.e., accidentally injecting the injectate into a vein or, even worse, an artery.
Specifically, the fluoroscopy machine (figure 8) uses a special low-level radiation to create a continuous radiographic picture of the low back—kind of like the one used at the airport for security screening.
During the ESI procedure, the physician will watch the monitors of the fluoroscopy machine in order to see exactly where the tip of that razor-sharp needle is, for even with fluoroscopy, it's not easy to place the needle precisely within the epidural space.
By using fluoroscopic guidance, not only is there an increased chance of properly placing the injectate, [8] but the chances of injuring the patient are greatly reduced. [9] Fluoroscopic guidance should always be used for ESI procedures, no matter which of the three approaches are used. [7]
Although using fluoroscopy during the ESI procedure may sound like a no-brainer, you would be shocked at the number of physicians who don't use it, and despite the rationale, they are truly doing you a disservice by cutting corners. Specifically, medical research has demonstrated that these "blinded" ESI procedures fail to get the injectate into the epidural space (i.e., the target) 30-40% of the time! [7,8] Furthermore, by not using fluoroscopic guidance (or CT guidance) the risk of minor and major procedural complications significantly rises. [9] Therefore, I would not allow any of my patients or myself to undergo ESI without fluoroscopic guidance. For an example, in some patients a fairly large artery may be present (it is called the Artery of Adamkiewicz), and if it is accidentally injected, then the patient runs the risk of developing serious catastrophic complications, such as spinal cord infarction, paraplegia, or stroke (all secondary to the injectate emboli that will wreak havoc wherever it goes).
Epidural Steroid Injections: Three Different Approaches
Caudal ESIs are performed by routing the needle through the narrow caudal canal of the sacrum and then releasing the steroid into the posterior epidural space (which of course is behind the thecal sac) only at the level of L5/S1. After its release the injectate must diffuse from the posterior epidural space, around the thecal sac, and (hopefully) enter the anterior epidural space in order to find its target: the disc herniation, annular tear, and/or inflamed nerve root. Although this technique is still useful for patients who have suffered a lot of scar tissue (perineural fibrosis) in the anterior epidural space from a previous spine surgery, it has anecdotally really fallen out of favor because of its limitations and therefore is not encouraged. [3,7,13]
Interlaminar ESIs (ILESIs) which are still commonly used today, involve putting the needle between the lamina (or through the supraspinous ligament) of the affected motion segment and then through the ligamentum flavum, which results in a "pop" and "loss of resistance" that the injectionist (doctor doing the procedure) can hear and feel. Like the caudal ESI, the injectate is released into the posterior epidural space and has to migrate around the thecal sac to the anterior epidural space in order to find its target. Some authors believe that it is "improbable" for the steroid to actually reach its intended target via this method and discourage its use. [7]
Transforaminal ESIs, which are very popular these days, involve placing the needle within the neural foramen of the affected motion segment, after which the steroid is released into the foramen and lateral anterior epidural space. The injectate now must travel only a short distance in order to reach the target; i.e., the inflammed nerve root, disc herniation material, and the posterior disc. (figure 7.6 & 7.9)
As noted above, there has been a 665% increased utilization of this procedure between the years of 2000 and 2011, [13] which is a significantly greater increase when compared to caudal ESIs or ILESIs.
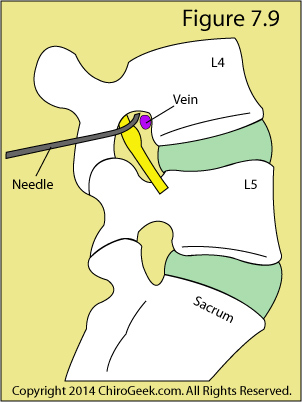
Figure 7.9 is a para-sagittal cartoon through the neural foramina that demonstrates the traditional needle placement for a transforaminal ESI. Note the good-sized vein that is in close proximity to the needle tip. Sometimes (especially on the left side) an artery of that size appears and increases the chance of inadvertent intravascular injection, which could be catastrophic. [11]
Now, perhaps you may realize why using fluoroscopic guidance is so important when performing ESIs. Even with the use of fluoroscopic guidance, inadvertent vascular penetration of the needle tip into the vein occurs in 7.4% to 11.2% of the patients; although, it is very rare for this accidental penetration to be in an artery, which typically is much more devastating than in a vain. [9] Luckily, because of the fluoroscopic guidance and epidurogram, the injectionist will soon realize that he has "poked" the vein and will reposition the needle accordingly, typically with no harm done.
Transforaminal Lumbar Epidural Steroid Injection: the new gold standard
Because of the long distance between the site of injection and the target, both interlaminar and caudal ESIs must use a significantly higher volume of steroid (typically ~9mL) in order to be effective. [4,6] Such a high volume of steroid can increase the risk for large spikes in blood glucose and blood pressure, which might not bode well for patients who are diabetic and/or hypertensive, and increase the risk of osteoporosis of the vertebral body.
On the other hand, because they are performed within or very near to the anterolateral epidural space, TFESIs use a much lower volume of steroid (typically ~3mL), yet they are just as effective, if not more effective, then the posterior epidural procedures. [5]
Personally, I have had both the interlaminar and transforaminal injections and, although they both eliminated back and leg pain, the transforaminal effect lasted much longer (one month) than the interlaminar injection (one week).
Although this is slightly beyond the scope of this webpage, I should mention that there are three different needle techniques or approaches to the target that can be used during a TFESI.
The most common is called a subpedicular approach and, like figure 7.9, places the needle above the nerve root. Although this technique places the needle closer to the vasculature of the neural foramen, it also allows for a better epidurogram, which can then be used to avoid accidental needlestick injury to those structures, as well as to the nerve root.
The retroneural approach places the needle tip more dorsally in the neural foramen and decreases the chance of accidental vascular injection. However, because this position results in a weak epidurogram, anecdotally the chances of nerve root stick may be higher.
The retrodiscal approach places the needle tip underneath the exiting nerve root and is a similar approach to that used during discography. Again, the chances of vascular injection are diminished, but the epidurogram is also weak; therefore, anecdotally, there is an increased chance of nerve root stick.
Volume Reaction Versus Nerve Root Stick
It is not uncommon, even with the use of fluoroscopy and epidurogram, for the injectionist to accidentally prick the exiting nerve root. Typically, this may result in an electrical-type pain traveling down the lower extremity and may well cause a flareup. If such a needlestick does occur, an immediate injection of lidocaine at the needlestick area should be performed in order to mitigate the magnitude of the flareup.
Anecdotally, some patients suffer a "volume reaction" to a ~5mL or greater volume of injectate that is believed by some injectionists to exert a mass effect upon the inflamed nerve root, which in turn results in intermediate flareup of lower extremity pain. This flareup typically settles down in a few days as the effects of the steroid kick in.
The Bottom Line
Based upon my research and my personal experience with epidural steroid injections, there's no question that they are useful in reducing severe sciatica and/or low back pain. However, their palliative (pain relieving) effect will probably not last for more than a month or two, after which the procedure needs to be repeated.
Even though the majority of the research seems not to support any long-term benefit of ESIs, anecdotally and logically I believe there is one. If you can get this procedure done soon after the start of sciatica, then the inflammatory process can be immediately reined in, which in turn may potentially prevent intraneural sequelae from an inflammatory process that otherwise is allowed to run amok.
Therefore, I am a believer in TFESIs for severe flareups at any time and their use to mitigate permanent lumbar nerve root damage if they are used quickly after the beginning of sciatica.
References
1) Parr AT, Diwan S, Abdi S. Lumbar interlaminar epidural injections in managing chronic low back pain and lower extremity pain: a systematic review. Pain Physician 2009;12:163-188.
2) Chou R, Atlas SJ, Stanos SP, Rosenquist RW. Nonsurgical interventional therapies for low back pain: a review of the evidence for an American Pain Society clinical practice guideline. Spine 2009;34:1078-1093.
3) Fetzer A, Scott DR. Nonsurgical treatment of herniated nucleus pulposus. In: Phillips FM, Lauryssen C, eds. The lumbar intervertebral disc. New York, NY: Thieme; 2010:86-91.
4) Manchikanti L, Cash KA, McManus CD, et al. A randomized, double-blind, active-controlled trial of fluoroscopic lumbar interlaminar epidural steroid injections in chronic axial or discogenic low back pain: results of two-year follow-up. Pain Physician to 13;16:E491-E504.
5) Rados I, Sakic K, Fingler M, et al. Efficacy of interlaminar versus transforaminal epidural steroid injection for the treatment of chronic unilateral radicular pain: prospective randomized study. Pain Medicine 2011; 12:1316-1321.
6) Parr AT, et al. Caudal epidural injections in the management of chronic low back pain: a systematic appraisal of the literature. Pain Physician 2012;15:E159-198.
7) Vad VB, Bhat AL, Lutz GE, et al. Transforaminal epidural steroid injections in lumbosacral radiculopathy: a prospective randomized study. Spine 2002; 27:11-16.
8) Weinstein SM, Herring SA, Derby R. Contemporary concepts in spine care: epidural steroid injections. Spine 1995; 20:184-186.
9) Karaman H, Kavak GO, Tufek A, et al. The complications of transforaminal lumbar epidural steroid injections. Spine 2011; 36:E819-E824.
10) Arden NK, et al. A multicenter randomized control trial of epidural corticosteroid injections for sciatica. Rheumatology 2005; 44:1399-1406.
11) Goodman BS, Posecion LWF, Mallempati S, Bayazitoglu M. Complications and pitfalls of lumbar interlaminar and transforaminal epidural injections. Curr Rev Musculoskelet Med 2008;1:212-222.
12) Andreisek G et al. Access routes and reported decision criteria for lumbar epidural drug injections: a systematic literature review. Skeletal Radiol 2013; 42:1683-1692.
13) Manchikanti L, Pampati V, Hirsch JA. Assessment of growth of epidural injections in the Medicare population from 2000 to 2011. Pain Physician 2013; 16:E349-364.
14) Novak S, Nemeth WC. Arch Phys Med Rehabil 2008; 89:543-552.
Home | Top