
The Disc Herniation Page
Not a big fan of reading? Check out my YouTube video on disc herniations: Lumbar Disc Herniations
Note: I strongly suggest that you visit the Disc Anatomy Page before diving into to this section of the website, for I am going to assume that you know a little bit about the general anatomy of the lumbar spine. Furthermore, since I will commonly use sagittal and axial MRI images as teaching tools, you might want to visit the MRI Page as well in order to get a handle on that subject.
YouTube Video: I've also created a YouTube video that highlights some of this material. It's not nearly as comprehensive as this page, but it will give you a good understanding of lumbar disc herniations. Watch it here: Lumbar Disc Herniations
Lumbar Disc Herniation: General Information?
In this first section, I'm not going to go too deep. Instead, I am just going to cover the major facts about disc herniation-this will be a great place for you to start learning about disc herniation. However, if you are a professional healthcare provider or student, make sure you read through the entire page, which goes much deeper into the subject matter.
Disc Herniation: the basics
 A disc herniation is a somtimes-painful condition of the spine that occurs when the material from the center of the disc (nucleus pulposus) escapes through an abnormal tear in the back portion of the disc (this is called an annulus fibrosus).
A disc herniation is a somtimes-painful condition of the spine that occurs when the material from the center of the disc (nucleus pulposus) escapes through an abnormal tear in the back portion of the disc (this is called an annulus fibrosus).
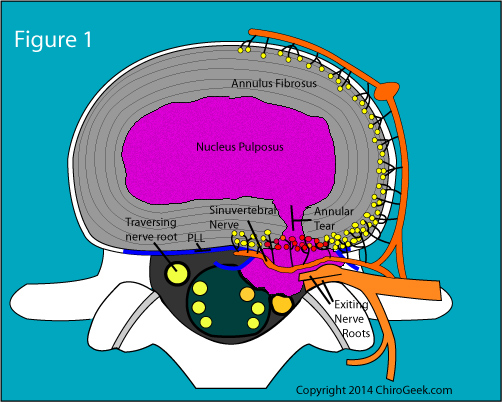
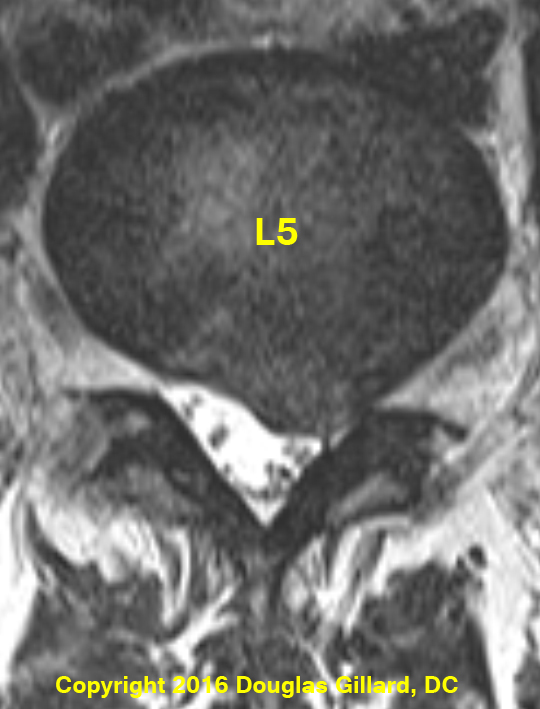
This out of place nucleus pulposus can then "poke" or "protrude" from the back of the disc and physically compress the adjacent nerve roots, nerve roots that make up the mighty sciatic nerve (or femoral nerve, depending on which disc is herniated). [Figure #1]
Figure #1 represents a disc-level axial (from underneath, so the sides are reversed) cut through the L4/5 disc that demonstrates a massive disc herniation (purple stuff outside of the disc) that was big enough compress both the exiting and traversing nerve roots. Note the posterior displacement (pushing back) of the left traversing nerve root. This patient would have horrible radicular pain (sciatica), with or without associated low back pain.
Although disc herniations can be completely asymptomatic (not a source of pain), [25] they can also produce debilitating lower back pain, with or without a burning, numbing, tingling, electric-like pain in the buttock and/or lower limb. These lower extremity unpleasant sensations are officially termed "radicular pain" or sciatica. (visit the sciatica page, for more information).
Note: from now on I will use the term radicular pain to describe that unpleasant/painful sensations that often accompanies disc herniation.
Why does the disc herniation cause low back pain? It is extremely important to understand that the low-back pain associated with the disc herniation comes from the annular tear that "gave birth to" the disc herniation. More Specifically, degenerative chemicals (cytokines and interleukins) move through the annular tear and then soak into the nerves that innervate the outside of the disc, which in turn sparks a low back pain-generating inflammation.
Why does the disc herniation cause radicular pain (i.e., an uncomfortable sensation down the buttock and/or lower extremity)? There are three possible causes of the radicular pain, which are both associated with the disc herniation:
#1 Physical Compression of the Adjacent Nerve Root: The mass of the herniation can physically smash either the traversing or exiting nerve roots, which are in very close proximity to the back of the disc. The contact will allow inflammatory chemicals (cytokines and chemokines) to soak into the nerve root and spark a pain-generating inflammation within that nerve root. Note: it is well known that without the inflammation, compression alone will not cause a radicular pain.
#2 Referred Pseudo-Radicular Pain: We all know that when someone suffers a heart attack, one of the first symptoms could be pain shooting down the left arm. There's nothing wrong with the left arm. The brain is getting confused by pain signals coming from the heart and misinterprets those signals as something wrong with the left arm. This is called referred pain. The same thing can happen with a symptomatic annular tear! Specifically, the inflamed nerves within the annular tear can send strong pain signals to the brain which then gets confused and believes the pain is coming from the buttock and/or lower extremity.
#3 Chemically Induced Radicular Pain: those same evil pro-inflammatory biomolecules (cytokines and interleukins) can physically "leak" out of the annular tear and soak into the adjacent nerve roots. Once the nerve roots become inflamed, that sets off the sensation of radicular pain. This may be in combination with the physical compression from the disc herniation or can occur with a very small disc herniation or even no disc herniation.
Classes of Herniation
The very first thing important to understand is that the word "herniation" is a parent category that has three children categories below it, Which include #1) disc protrusion (a.k.a., contained herniation or subligamentus herniation); #2) disc extrusion (a.k.a., non-contained herniation or transligamentous herniation) and sequestration (a.k.a., fragment or free fragment). We will talk more explicitly about each one of these here.
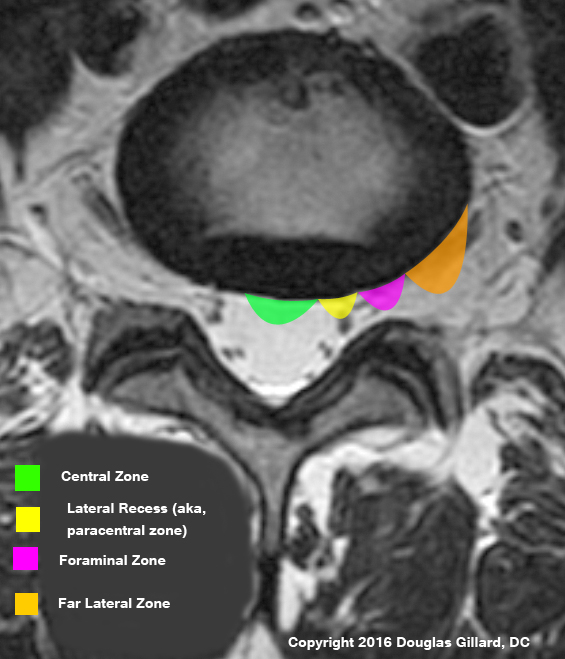
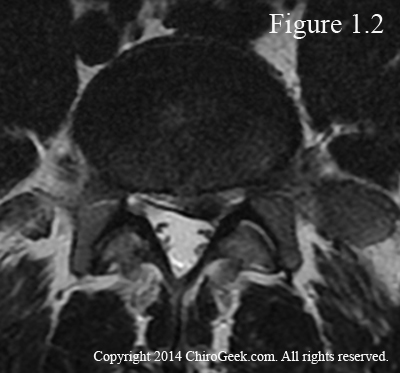 Disc herniations are also described by their location as visualized on axial (from underneath) imaging. Specifically, if we use the disc as a clock-reference (6 o'clock would be dead-center posterior), a central disc herniation would be exactly at the 6 o'clock position; a paracentral disc herniation (figure 1.2) would be at the 7 or 5 o'clock position; a foraminal disc herniation, which occurs within the neural foramina, would be at the 8 or 4 o'clock position; and a far lateral disc herniation would be located lateral to the foraminal disc herniation. Here is a popular picture that I use in my lumbar differential diagnosis II class. Disc Herniation Zones
Disc herniations are also described by their location as visualized on axial (from underneath) imaging. Specifically, if we use the disc as a clock-reference (6 o'clock would be dead-center posterior), a central disc herniation would be exactly at the 6 o'clock position; a paracentral disc herniation (figure 1.2) would be at the 7 or 5 o'clock position; a foraminal disc herniation, which occurs within the neural foramina, would be at the 8 or 4 o'clock position; and a far lateral disc herniation would be located lateral to the foraminal disc herniation. Here is a popular picture that I use in my lumbar differential diagnosis II class. Disc Herniation Zones
{kind=link}
Figure 1.2 is a T2-weighted MRI image of the L4 disc. Can you see the left, broad-based paracentral disc extrusion, which is about 6 mm in size? If not, click here. The arrows will be pointing out the herniation.
Although foraminal and far lateral disc herniations are not seen as often as central and paracentral herniations are, when they do occur, they are often trouble, for they don't typically respond well to conservative or even operative care.
 .
.
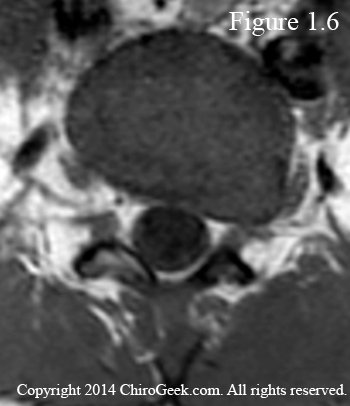
Figure 1.6 at T1-weighted MRI image through the L4 disc that demonstrates a massive far lateral disc herniation on the left. In fact, it is so large that it invades the neural foramen as well. Can you see it? If not, click here.
Furthermore, if a disc fragment moves into the far lateral position it is sometimes missed on MRI.
And if it is not seen on the MRI, then it may be missed during discectomy, for the surgeon will probably not be looking at it. This is especially true if the surgeon is using one of the endoscopic techniques which significantly lessens his or her field of vision.
Strange Fact about Disc Herniations:
Although you would think that the larger the disc herniation, the more severe the symptoms, this does not appear to be true. Specifically, we learned from Karppinen et al. that the size of the herniation has nothing to do with the amount (quantity) of pain or disability of the affected person experiences. [170] In other words, size does not matter, for the tiny contained herniation can result in just as much patient-suffering and disability as the giant sequestration. [170]
Disc Herniation: Making the Diagnosis
The working diagnosis of disc herniation is made when a patient presents (is evaluated by the doctor) with complaints of low back pain and/or radiating lower limb pain that are associated with positive examination findings (especially a positive Lasegue's test and/or positive neurological findings).
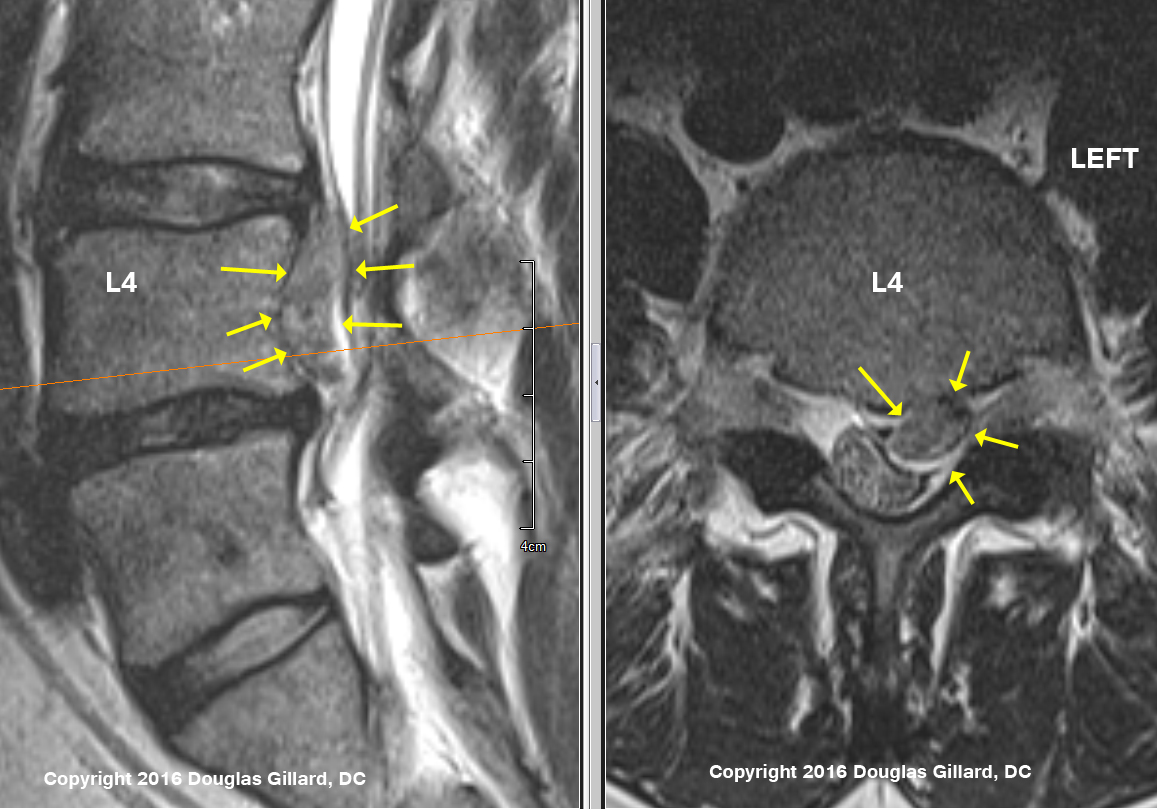
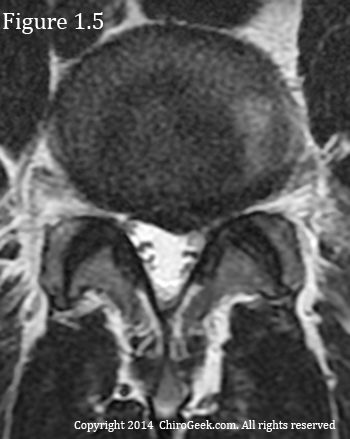 Magnetic resonance imaging (MRI) findings that demonstrate a focal or asymmetric outpouching of the posterior or posterolateral disc margin (especially at L4 or L5) will strengthen the diagnosis of symptomatic disc herniation. (figures 1.5, & 2)
Magnetic resonance imaging (MRI) findings that demonstrate a focal or asymmetric outpouching of the posterior or posterolateral disc margin (especially at L4 or L5) will strengthen the diagnosis of symptomatic disc herniation. (figures 1.5, & 2)
Figure 1.5 is a T2-weighted image of an L4 disc which has suffered a symptomatic left-paracentral protrusion that caused significant left lower extremity pain and weakness of the foot dorsiflexors. Do you see the compressed and swollen left L5 nerve root? If not, click here. The arrows point out the herniation, and I have circled the traversing L5 nerve roots.
However, you have to be very careful when interpreting MRI results, for it is well-established that approximately 30% of middle-age people will have a protrusion on MRI, yet have no history of back or leg pain. In other words, MRI has a ~30% false positive rate when it comes to detecting disc protrusions. [25,95,97] (*MRI is much more accurate for detecting disc extrusions or sequestrations.)
To really strengthen the diagnosis, a test called electromyography (EMG) can be ordered if there is MRI evidence of disc protrusion in association with patient-complaints of radicular pain and positive neurological findings on examination. (We shall discuss this test further below.)
Disc Herniation Treatments:
Conservative Care
Osteopaths, chiropractors, physical therapists, and acupuncturists are always the first line of defense against a symptomatic disc herniation, with or without radicular pain (sciatica). Although I'm not going to get into the details of each specific type of care, I do want to warn the disc herniation patient about trying grade 5 (twist and crack the bones) spinal manipulation for disc herniation. I've consulted with many patients over the years who've been worsened by this violent twisting and cracking of the vertebral column and therefore strongly recommend this not be done for patients with symptomatic disc herniations. There are, however, more gentle techniques that could be tried, such as decompression, Cox flexion/distraction, and Mulligan's spinal mobilization techniques. [footnote coming]
Prescription medication has also been demonstrated to be quite effective at battling lumbar disc herniation and should be considered as part of a multidisciplinary approach.
Fluoroscopic guided epidural steroid injections should be considered if the above-mention conservative care fails. Research has supported their efficacy, at least in the short run.
Discectomy Versus Fusion
Discectomy
If the symptoms of disc herniation have improved over the initial 3 months post-onset, and are continuing to improve, then typically no surgical intervention is necessary. [74] However, for the people who are refractory (didn't improve) to non-operative care (i.e., activity modification, bracing, physical therapy, medication, injective procedures, low-force chiropractic, and acupuncture) and continue to suffer radicular pain as a major complaint, a spine surgery called a discectomy is typically necessary to remove the herniation in hopes of breaking the compression, inflammation and pain cycle.
 Does discectomy work? Without digging too deep into this very complex question, which we will discuss in great detail farther below, the short answer is typically yes, in the short run (<1-2years) [13,74,81] and maybe in the long run (10 years). [13]
Does discectomy work? Without digging too deep into this very complex question, which we will discuss in great detail farther below, the short answer is typically yes, in the short run (<1-2years) [13,74,81] and maybe in the long run (10 years). [13]
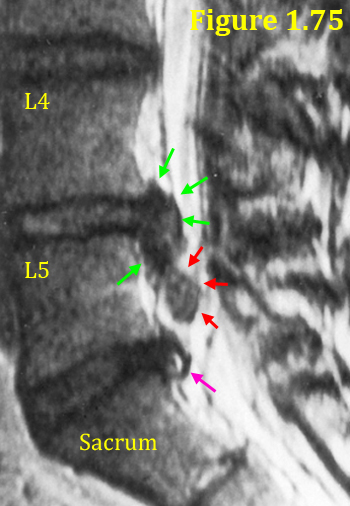
In Figure 1.75, is a T2-weighted sagittal MRI image through the lumbar spine that demonstrates a rare type of disc herniation called a sequestration. A sequestration occurs when a fragment of herniation (red arrows) breaks off from the main disc extrusion (green arrows) and is free to travel within the epidural space.
*What is the pink arrow pointing at? It is pointing to a small contained disc herniation at L5/S1 that has indications of an annular tear within it. Do you see the HIZ sign?
Here is another pitfall that you must know (I wish I would have known this fact before I had my discectomy, which failed miserably):
Discectomy has a much higher success rate when the surgery is performed on a herniation that is at least 8 mm in size and has an absolutely horrible success rate for herniations that are less than 5 mm in size. [22] *The foregoing claim was based upon the results of a very well done Stanford discectomy study that looked at disc herniation morphology. [22] I shall discuss this in much more detail below.
Interbody Fusion
For disc herniation patients with low-back pain greater than radicular pain, discectomy does not work very well and, anecdotally, you probably have less than a 50% chance of the discectomy working. [107] This is most likely due to the fact that discectomy fails to address the pain-generating annular tear inside the disc, which is believed to be responsible for the low back pain associated with disc herniation. Therefore, lumbar interbody fusion is probably a better option; however, fusion is always a last-resort treatment and the patient must have exhausted all other options.
 So, what do you do if you have a disc herniation on MRI, but your low back pain is much greater than the lower limb pain?
So, what do you do if you have a disc herniation on MRI, but your low back pain is much greater than the lower limb pain?
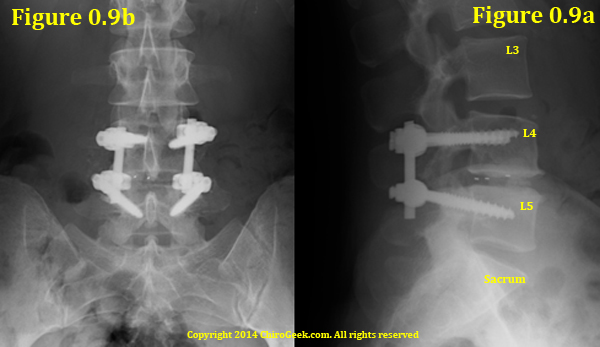
Figure 0.9 is an AP (0.9b) and lateral (0.9a) radiograph of a typical transforaminal lumbar interbody fusion, which was performed on this patient because she had had three prior recurrent disc herniations at the same disc level.
Unfortunately, the best available treatment (based upon the medical literature) at the time of this writing (2014) is interbody fusion, which removes the disc herniation, nucleus pulposus, and some of the annulus and then fuses the affected motion segment into one unit. Please visit my Fusion Page for more information.
Fusion, on the other hand, is a "last-ditch effort" to help someone with severe disabling back pain and should never be attempted, in my opinion, unless the patient scores well over 50 on the Oswestry Disability Index.
Experimental Procedures
If you are a risk taker, however, then there are several other treatment options (which continue to be deemed "experimental" via the major insurance companies, and I would have to agree ) that include IDET, SED, Nucleoplasty, Prolo-therapy, Disc Biacuplasty... and the list goes on.
If I were superrich (these typically are not covered by insurance) and wanted to try one of these treatments as an attempt to avoid fusion, which one would I try? It really depends on your unique situation, and therefore cannot comment here. However, I would be more than happy to discuss this further with you via a Coaching Session.
Natural History: Don't Do Anything
Typically, as long as you don't have "red flag" (emergency) indications (i.e., bowel/bladder dysfunction, progressive neurological deterioration, excruciating pain, or perineal sensory loss) for surgical removal of the disc herniation, you can typically let "mother nature" do her thing. Although this topic is highly debatable, medical research, both past and present, seems to indicate that with regard to satisfaction patients who have discectomy within ~6 months (within 12 months at the very most),are typically quite pleased with the results. Patients who don't have discectomy, on the other hand, are typically miserable. However, with the passage of time (and I mean a lot of time), the patients who didn't have discectomy tend to "catch" the patients who did had discectomy within about 4 years. [Weber-1982 (Volvo Award-winning)]
Evidence-Based Facts and Figures
What are the risk factors for the development of a disc herniation? Although there is some evidence that genetics, vibration, non-occupational lifting, [92] vertebral endplate shape, [94] and sedentary work [74] may increase the chances of developing a symptomatic disc herniation, the greatest risk factor appears to be working a very physical job (so strenuous that you sweat almost every day) that involves activities such as repeated bending, twisting, stooping, and/or heavy lifting. [93]
What are the chances that you will develop a symptomatic disc herniation over the working years of your life? Although, very few studies have looked at the general population to make this determination (which is how it should be done), [98] one very large study came close. After analyzing the data from 3,833 middle-aged workers, who were employed in many different industries and initially had no history of back or leg pain, the research team reported that over the 30-year study period, 1.7% of the workers suffered a severely symptomatic disc herniation, which landed them in the hospital. [98] *Anecdotally, I think the number of symptomatic herniations in the population would be higher than this, for many people who suffer these herniations do not report to the hospital for care. [93]
What are the odds that you may need disc surgery because of a symptomatic disc herniation? Again, surprisingly, there is not much research on what percentage of the population require spine surgery for a herniated disc. However, one investigation did study the incidence (how many people got the surgery over a given time period) of discectomy in an initial population of 48,228 people (an entire city), who were only serviced by one hospital. After analyzing 30 years worth of data, the researchers concluded that 1.95% of the population underwent a discectomy for symptomatic lumbar disc herniation during that study period. [105]
Okay, that pretty much covers the basics of lumbar disc herniation. if you want to read more about treatment, jump down to here.
Now let's really dig into the subject matter.
Disc Herniation: How to Make the Diagnosis
*In order to make sure that you are not misdiagnosed, which could potentially result in an unnecessary and failed spine surgery, it is important to read and understand this section thoroughly, for many physicians just don't understand the simple algorithm I am about to present!
Warning: Diagnosing a Symptomatic Disc Herniation is Not as Simple as You Think!
Before continuing on, I must warn you that diagnosing a symptomatic disc herniation can be very tricky, for it is well known that nothing in the world of Spine is 100% for sure, and there are always exceptions to any rule. For example, sometimes a tiny contained disc herniation can result in horrible sciatica and even demonstrate positive EMG/NCV testing, yet on MRI there is no evidence of nerve root compression. Other times, a massive disc extrusion can result in very little lower extremity pain, even though it is smashing the nerve roots on MRI. Stranger still is the phenomenon of a patient with horrible lower extremity pain and associated full-blown EMG/NCV-confirmed radiculopathy, yet the MRI is completely normal. Or maybe a patient with a perfect EMG/NCV-confirmed S1 radiculopathy learns that the leg pain is being caused by a tumor compressing the nerve root. Get the point? Never tried to diagnose yourself without the help of a qualified healthcare provider!
If you or your doctors are confused about the cause of your pain and/or what to do about it, then why not let me help you figure things out.
I offer a Coaching Service for situations like this, during which you and I will go over your images together via GoToMeeting and then formulate an evidence-based action plan based the medical literature database.
If you are interested, please click the following links to learn more about this popular service. Coaching Session with Dr. Gillard | What Are My Clients Saying (Testimonials)
The diagnosis game begins with a comprehensive (detailed) examination by your healthcare provider. Particular attention should be paid to the presence of lower extremity (lower limb) neurological findings such as sensory change, motor weakness (a weakness and/or atrophy in a nerve-specific muscle group), and/or reflex alteration. An orthopedic test called Lasegue's test (aka, straight leg raise test) is also fairly important and is one of the rare noninvasive ways to diagnose the disc herniation. [170]
*If you have signs of bowel and/or bladder dysfunction (i.e., you have lost control of your poop and/or pee), then you have a medical emergency on your hands and need to get to the emergency room immediately so that an MRI can be ordered. The fear is that you may have developed cauda equina syndrome secondary to something (usually a large disc extrusion or sequestration) severely compressing the thecal sac, which in turn is irritating the extremely delicate nerve roots that supply the bladder and rectum. Putting off this trip to the ER, may result in unrepairable nerve damage and life-long bowel/bladder dysfunction.
 If there are complaints of lower back pain with associated radicular pain (especially if that lower limb pain travels from the buttock past the knee), as well as positive neurological findings upon examination, then a special test called an MRI should be ordered sooner rather than later. *MRI is the only test that can actually visualize (see) the disc herniation. (figure 2) Although computed tomography (CT) can faintly make out the outline of a herniation, it is not intended for viewing soft tissue structures, such as the disc, and the two-dimensional x-ray (radiograph) is completely incapable of seeing the herniation.
If there are complaints of lower back pain with associated radicular pain (especially if that lower limb pain travels from the buttock past the knee), as well as positive neurological findings upon examination, then a special test called an MRI should be ordered sooner rather than later. *MRI is the only test that can actually visualize (see) the disc herniation. (figure 2) Although computed tomography (CT) can faintly make out the outline of a herniation, it is not intended for viewing soft tissue structures, such as the disc, and the two-dimensional x-ray (radiograph) is completely incapable of seeing the herniation.
Figure left is a T2-weighted mid-sagittal MRI image that demonstrates a large L4 disc extrusion within the anterior epidural space (may be a sequestration). Note how the posterior and superior nuclear material (nucleus pulposus) of the fragment is starting to reabsorb (lighter in color) compared to the main body of the disc.
Electromyography & Nerve Conduction Velocity Testing
Another important test that should not be overlooked for patients with radicular pain and positive neurological findings on exam is called electromyography (EMG).
Electromyography, which should be accompanied by a nerve conduction velocity study (NCV), has the unique ability to detect nerve-root-level axon damage (damage to the tiny nerve fibers that makeup the nerve root) and will really finalize the diagnosis of disc-herniation-related radicular pain if found to be positive. This test also has the ability to differentiate between disc herniation-related sciatica and other causes of sciatica (e.g., diabetes and herpes zoster), as well as differentiate between acute and chronic radicular pain.
 *If the EMG is positive (i.e., there are indications of denervation {axon death} via increased insertional activity, positive sharp waves and/or fibrillation potentials), then the patient is said to have radiculopathy, which means that the radicular pain has most likely occurred from the dead and dying large-fiber myelinated axons within the nerve root. In other words, the nerve root that is adjacent to the disc herniation is really messed up.
*If the EMG is positive (i.e., there are indications of denervation {axon death} via increased insertional activity, positive sharp waves and/or fibrillation potentials), then the patient is said to have radiculopathy, which means that the radicular pain has most likely occurred from the dead and dying large-fiber myelinated axons within the nerve root. In other words, the nerve root that is adjacent to the disc herniation is really messed up.
One of the pitfalls of EMG/NCV is its low sensitivity, which means that it misses a lot of true cases of radiculopathy (high false-negative rate). However, because of its very high specificity—when it finds radiculopathy, you really have radiculopathy (very low false-positive rate)—it is definitely an important tool for really nailing down the diagnosis of disc herniation-related radicular pain and should always be ordered for a patient with lower extremity pain and positive neurological findings.
*The test is also time-sensitive and should never be performed less than four weeks from the onset of the radicular pain. In other words, if it is performed too early, it will almost always be completely normal, for it takes time for the damaged axons to affect the muscles that will be tested by the procedure. (**Case and point: I was recently evaluated by a pain management doctor (a physiatrist) here in the bay area for the purpose of medication refill, and to my surprise she wanted to perform an EMG/NCV on me, notwithstanding the fact that my sciatica flared-up had only just happened two weeks prior! I politely declined and educated her {which of course annoyed her greatly}. Did she not know the physiology of EMG/NCV? Or was she just trying to increase her bottom line? You have got to know this stuff people!)
And, I almost forgot, one other pitfall: the EMG/NCV study does not test the nerves that actually carry the signals of pain (i.e. the small non-myelinated C-fiber); it only tests the large myelinated motor nerves.
Okay, I can hear you. You are saying , "What is the point of suffering through this painful study when it doesn't even test the pain-carrying nerve fibers?" The smaller pain-carrying nerve fibers are in very close proximity to the larger myelinated nerve fibers which are tested. Specifically, all of the flavors of nerve fibers are are tightly bundled within the exiting or traversing nerve root, which in turn are encased within the dural sleeve. Therefore, if the large myelinated fibers are damaged, you can bet your bottom dollar that the small non-myelinated pain fibers are damaged as well. *There are, however, some conditions that only affect the small non-myelinated nerve fiber, but that is beyond the scope of this page.
Disc Herniation: What Causes the Pain?
Since a disc herniation can cause both low back and/or lower limb pain, let's address each one of these pain syndromes separately.
What Causes the Low Back Pain? The Annular Tear
It is important to understand that when the disc herniation compresses the adjacent nerve root, the irritated root is not responsible for the symptoms of low back pain. The nerve root compression, in at least part, is responsible for the lower limb pain, which we will talk about further below. [32,80,95,96]
 So, if the compressed nerve root is not causing the back pain, what the heck is?
So, if the compressed nerve root is not causing the back pain, what the heck is?
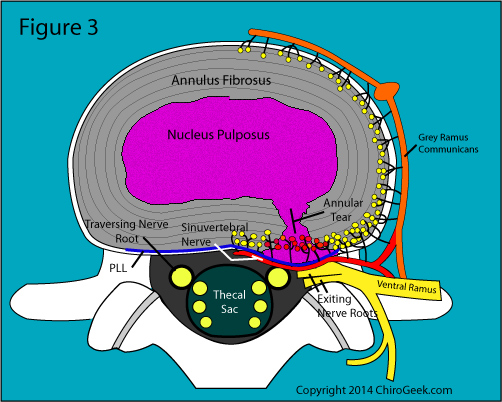
It is believed that the channel between the center and periphery of the disc, which is called an annular tear, is responsible for the low back pain associated with disc herniation. [32,80] (figure 3) (Learn more about annular tears)
Figure 3 is an axial view through the disc-level of the lumbar motion segment. Note the full-thickness annular tear that has resulted in a focal or asymmetric outpouching (a bump) of the posterior disc margin within the left lateral recess and neural foramen (left side of picture). Because this herniation is contained by the posterior longitudinal ligament (PLL), it is classified as a contained disc herniation or protrusion.
More specifically, the annular tear is thought to cause low back pain via three mechanisms: inflammation, mechanical irritation, and autoimmune-related inflammation.
Let's take a look at each mechanism. (*Warning: a lot of this information may be too complicated for the layperson; however, if you are a medical, physical therapy, or chiropractic student who wants to specialize in the spine, then it is quite important that you understand these concepts.)
#1) Inflammation of the Sinuvertebral Nerve Nociceptors
The full-thickness annular tear of a disc herniation will obviously allow the pressurized nucleus pulposus (nuclear material) to enter and come in contact with the pain-triggering nociceptors (yellow and red dots on figure 3) of the sinuvertebral nerve.
This invasion of nucleus pulposus may result in the development of an inflammatory process that triggers the nociceptors to transmit pain signals to the brain, which of course interprets these signals as the sensation of pain.
*The specific pain path is thought to be as follows: the pain signals leave the nociceptors, travel across the sinuvertebral nerve, move anteriorly through the gray ramus communicans (orange, figure 3) and into the sympathetic trunk where they probably travel up to the L1 or L2 spinal ganglion. Then they travel back to the ventral ramus (probably at L1 or L2), enter the spinal cord, and finally travel up to the sensory cortex of the brain.
If you are wondering why nucleus pulposus triggers an inflammatory reaction, I'll tell you, but you're going to be sorry you asked.
The Evil Biochemicals
It has been known for several decades that certain "evil" pro-inflammatory (inflammation-starters) biochemicals, such as prostaglandins, leukotrienes, thromboxane, nitrous oxide, cytokines (IL-1, IL-6, TNFa, and IFNy), as well as certain white blood cells (macrophage and lymphocytes) are contained within the nucleus pulposus—especially degenerated nucleus pulposus. [76]
If these biochemicals get loose in the posterior one third of the disc via an annular tear (recall that the posterior one third of the disc is the only region that contains the nociceptors of the sinuvertebral nerve and blood vessels), then a terrible inflammatory process may begin, which in turn causes the nociceptors to fire-off pain signals across the sinuvertebral nerve, which ultimately end up in the brain.
The $64,000 Question
Oh but it's not that simple! You see for reasons not completely understood, not all people develop an inflammatory reaction in and around the nociceptors after exposed to these biochemicals. Why? That is one of Spine's $64,000 questions, the answer to which we just don't know. However, it has been postulated the density (amount of) of nociceptors in the posterior annulus might vary amongst people. [32] For example, one person might have 50,000 nociceptors and be symptomatic, while another person might have 5000 nociceptors and therefore feel no pain at all. Or perhaps there is a yet-to-be-discovered anti-inflammatory biochemical that is present in some discs but not others. [32] Or this inflammation might be the result of an autoimmune reaction (I will explain this further below), the degree of which could be dependent on the person's unique description of "self." Figure out this enigma, and you will win a Nobel Prize for sure.
#2) Mechanical Irritation of the Sinuvertebral Nerve Nociceptors
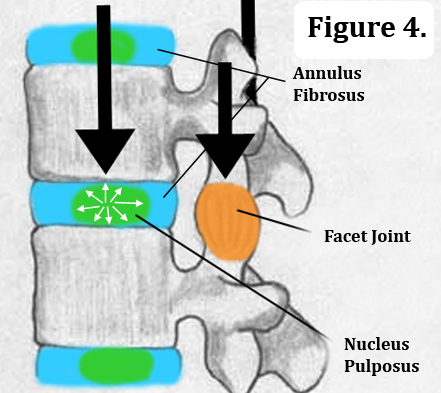 Recall from the Disc Anatomy Page that a normally functioning nucleus pulposus acts as a closed hydraulic system and efficiently transfers the downward axial load of the body and gravity (figure 4, black arrows) from the center of one disc, to the center of the next disc, and so on. (*The facet joints also help out the axial load.)
Recall from the Disc Anatomy Page that a normally functioning nucleus pulposus acts as a closed hydraulic system and efficiently transfers the downward axial load of the body and gravity (figure 4, black arrows) from the center of one disc, to the center of the next disc, and so on. (*The facet joints also help out the axial load.)
In a normal disc, the nucleus also acts as a pivot-point for all trunk motion (flexion, extension, lateral bending, and rotation), and its center location spares the innervated posterior annulus from undue mechanical irritation from such movements.
However, when an annular tear occurs, that beautiful hydraulic system is destroyed, which in turn allows the major disc compressive forces (i.e., the axial load and the pivot-point forces for trunk motion) to shift posteriorly (backwards) and onto the sensitive posterior annulus fibrosus. [82] (figure 4a)
Now, in addition to the biochemically-induced inflammation of the nociceptors, we get a biomechanically-induced (physical) irritation of the nociceptors because of the posterior axial load shift. Such a scenario results in the creation of a vicious cycle of mechanical irritation, inflammation, and pain generation.
#3) Autoimmune Irritation
Although I could have grouped this topic under inflammation, for ultimately an autoimmune reaction results in inflammation, I decided to make this a separate topic, for it is a fascinating theory which is somewhat supported by medical research [77,78,91] and is one possible explanation as to why some people suffer severe low back pain secondary to disc herniation and others don't.
The theory goes like this: since the cells of the nucleus pulposus were born into a completely avascular environment (there are no blood vessels in the center of the disc), the body's immune system, which basically lives in and around the bloodstream, is unaware of their existence and these cells are not recorded as "self." Therefore, when nucleus pulposus cells suddenly come in contact with the blood vessels of the posterior annulus via an annular tear, the body sounds an alarm that a foreign invader has entered and the immune system attacks. This attack ends up producing many of the same "evil" biochemicals that I have previously mentioned and will trigger a full-blown inflammatory process in and around the nociceptors, which in turn triggers pain signals to be sent to the brain via the route described above. [77,78,91]
This autoimmune theory may help to answer the $64,000 question of why some annular tears are painful and other annular tears are not. Specifically, perhaps some people's immune systems were "somehow" exposed to nucleus pulposus cells early in life and therefore recognize these cells as "self." If that were true, then the nuclear cells would not trigger a painful inflammatory process after the development of a full thickness annular tear, because they are recognized as self. We need continued research in this area! *Why is it not being done? Because in my humble opinion it boils down to money: if it is the immune system that is causing this inflammation, then we already have the drugs to fight it. That is, the same immunosuppressive medication available right now would be the treatment. Therefore, since the drug companies can't develop and patent any new medication (patenting new drugs is where they make their money), why bother to shell out research dollars?
The Research
There are two famous human studies that have demonstrated the region of the posterior annulus adjacent to the disc herniation does in fact result in the sensation of low back pain when stimulated. [32,80] I will discuss these in detail further below.
What Causes the Sciatica? The One-Two Punch of a Herniation
We are about to enter a fairly complex topic (one that is also covered on the sciatica page), so hang onto your hats and let's get rolling.
Based upon the current medical literature, "typically" (remember there are always exceptions to the rules of Spine) the lower extremity pain associated with disc herniation results from a combination of two phenomena: [32,79,80,84] (1) the mechanical (physical) compression (or at least contact) of either the traversing (more common) and/or the exiting nerve root by the herniation, [96] and (2) the inflammation of that nerve root secondary to a biochemical exposure. [85]
How do we know compression and inflammation are both typically needed to manifest sciatica? We turn to the medical literature. (Sorry, I have to talk about these two landmark human studies!)
The Research
 Smyth [80] was the first surgeon to demonstrate a connection between disc-herniation-related compression, inflammation, and radicular pain way back in 1958. Specifically, after removing the disc herniations from 37 patients suffering sciatica, he gently tied a nylon string around the affected nerve root, exactly over the site of compression (this root was often swollen at the site of herniation contact) and then closed the surgical wound with the end of the strings hanging out.
Smyth [80] was the first surgeon to demonstrate a connection between disc-herniation-related compression, inflammation, and radicular pain way back in 1958. Specifically, after removing the disc herniations from 37 patients suffering sciatica, he gently tied a nylon string around the affected nerve root, exactly over the site of compression (this root was often swollen at the site of herniation contact) and then closed the surgical wound with the end of the strings hanging out.
Figure 5 is a T2-weighted MRI image through the disc-level of the lumbar spine. As you should be able to see by this point, there is a small right paracentral disc herniation that is contained by the posterior longitudinal ligament. Can't see the herniation? Click here for the answer.
Approximately 2 days following the surgery and after the sciatica was gone in all patients, the strings were very gently tensioned so that the previously-compressed nerve roots (deep inside the spine) would be slightly moved. The team was very careful not to cause tension on the nerve root by pulling the string too hard—all they did was move it a few millimeters. Surprisingly, even though the nerve root was no longer compressed by the disc herniation, that slight pull of the string resulted in the re-creation of that same horrible pre-operative radicular pain in all the patients. [80] So, why did this slight nerve movement re-create the sciatica when the compression from the herniation had been removed? The logical answer would be that the nerve roots were still inflamed and sensitive to even the slightest compression by the string. In other words, compression and inflammation must go hand-in-hand with regard to the manifestation of sciatica. Animal research has also confirmed that physical compression of the nerve root does in fact result in pain-producing changes away from the side of compression (i.e., in the dorsal root ganglion and dorsal horn of the spinal cord). [96] *In one case, Smyth also looped the nylon string through the posterior annulus and discovered that the pulling of that string even a week after successful surgery re-created that patient's severe low back pain.
Smyth's results were confirmed in 1991 by Kuslich et al. [32] who reported on the intraoperative (during the surgery) findings of 193 patients undergoing spine surgery for nerve root compression that was caused by either a disc herniation or stenosis. The key to this study was that these patients were not put under via general anesthesia! That's right, Kuslich used layers of locally-applied lidocaine to numb these patients up. Therefore, they were able to verbally communicate with the surgeon during the operation and answered questions about what they felt after various anatomical structures (which included the affected nerve root, as well as the normal nerve root) were "stimulated." This stimulation was accomplished by gently pinching the structures with forceps, compressing them with blunt surgical instruments or shocking them with low volt electricity. After studying the data, the team reported that by stimulating the previously-compressed nerve root (the one that had just been decompressed by the surgery), nearly all patients (99%) suffered an immediate flare-up of the same radicular pain that they were on the operating table for. On the other hand, when the normal nerve root on the other side of the spinal canal was stimulated, none of them had pain. In fact, they had to compress the normal nerve root extremely hard and leave it compressed for several minutes before the patients finally developed a very mild thigh pain. *Interestingly, when the posterior annulus was stimulated adjacent to the herniation, 73% of the patients experienced a low back pain that was very similar to the type they had previously suffered. However, none of them experienced a re-creation of their radicular pain; [32] these findings were also reported by Smyth. [80]
Let's look a little more closely at each of these factors.
Disc-Herniation-Induced Nerve Root Compression
There is no question that nerve root compression by a disc herniation, which is inextricably associated with an inflammatory process, is related to radicular pain. [32,80,90,96] Furthermore, there is direct evidence that the magnitude (the amount of) of compression imparted onto the nerve root is directly related to the severity of neurological deficit experience by the patient. [90] In other words, the more pinched the nerve root is, the more damaged it will become.
How Does the Compression Affect the Nerve Root?
As you may recall from the disc anatomy page, the nerve roots, which are made up of thousands of nerve fibers called axons, have a tiny built-in circulatory system that is complete with veins and arteries. Just like any living tissue, these tiny axons need nutrients and oxygen (which come from the arteries), as well as a means to get rid of their waste (the veins) in order to survive. The cerebrospinal fluid (CSF) which percolates around the nerve roots (remember, the nerve roots are wrapped in a dural sleeve that is open to the CSF-containing thecal sac proximally) is another vehicle for nutrition and waste removal.
The nerve root, which lacks the protective perineurium that peripheral nerves have, [89] can only take so much compression and still remain healthy.
 If the magnitude of compression exceeds a certain limit (this limit may be different in everyone), then the nerve root's circulatory system will be compromised (stop working properly) and the axons will get "cranky" as they hunger for oxygen and other nutrients.
If the magnitude of compression exceeds a certain limit (this limit may be different in everyone), then the nerve root's circulatory system will be compromised (stop working properly) and the axons will get "cranky" as they hunger for oxygen and other nutrients.
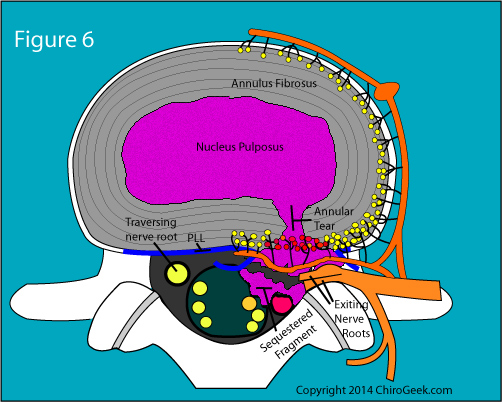
Figure 6 is an axial cut through the disc which demonstrates the worst type of disc herniation: a sequestration. Note that the sequestered fragment has broke loose from the main extrusion and is severely compressing the traversing nerve root as well as the thecal sac.
Furthermore, without the venous system working, there would probably be a build up of lactic acid, which would irritate (burn) the starving axons. There would also be diminished CSF flowing around the nerve root, so this vehicle for nutrition and waste removal would also be disturbed. So, what happens if the nerve root gets cranky? It inadvertently fires off its message to the brain or lower extremities–keep reading.
There is also fairly strong evidence that suggests both the dorsal root ganglion and the dorsal horn of the spinal cord (the beginning and end of the central process of the nerve root, respectively) are deleteriously affected from compression of the mid-point of nerve root (which occurs in all cases of herniation and stenosis), notwithstanding the fact that these regions haven't been physically compressed. [96] Specifically, Kobayashi et al. (2005) reported that compression of the nerve root adjacent to the lumbar disc in dogs (which was done with surgical clamps of varying strength) caused a build up of pain-producing neurotransmitters adjacent to the site of compression, and negatively affected the dorsal root ganglia and the dorsal horn of the spinal cord. The team concluded that this change in neurotransmitters could explain the radicular pain in patients with disc herniation. [96]
So, if these axons become distressed from compression, what do they do? Besides the obvious (they could die), some may begin to spontaneously fire their message to the brain (if they are sensory fibers) or to the lower extremities (if they are motor fibers). These inadvertent signals may cause symptoms such as lower extremity numbness, tingling, and/or radicular pain; muscle twitching and/or weakness; and/or reflex change. An interesting fact about the radicular pain (remember bundled with in the dorsal component of the lumbar nerve root are the tiny unmyelinated pain-carrying C fibers) is that although the irritation of the nerve root happens in the low back, your brain interprets those incoming pain-signals as coming from your lower limb (usually in a dermatomal pattern). In other words, the brain gets faked-out and thinks the nerve damage is within the lower limbs, when in reality it's in the low back.
Disc-Herniation-Induced Nerve Root Inflammation
As previously mentioned, the evil inflammation-starting biochemicals (i.e., prostaglandins, leukotrienes, thromboxane, nitrous oxide, cytokines {IL-1, IL-6, TNFa, and IFNy}), as well as certain white blood cells (macrophage and lymphocytes) are contained within the degenerated nucleus pulposus that escapes the center of the disc during disc herniation. [76] Because the disc herniation contacts or even compresses the adjacent lumbar nerve roots, these biochemicals can freely diffuse into the nerve root (as well as into the epidural space), [85] which in turn may create a rip-roaring, pain-generating inflammation in some, but not all patients. [88]
Just like compression, nerve root inflammation may cause spontaneous firing and even death in some of the axons (sensory and/or motor) at the level of herniation. And, as we have previously learned some of these axons will most likely have nociceptive (pain carrying) function. Therefore, this spontaneous firing of the nociceptive axons will inadvertently transmit signals of pain to the brain, which interprets them as coming from the dermatomes of the lower extremity and not the low back.
Okay, that is all the time I can put into revamping this page. Although kind of a mess, I will leave the forthcoming material here, because it is quite instructive even though I could certainly write this better.
Disc Herniation Classifications: protrusion, extrusion, & sequestration
Disc Protrusion | Disc Extrusion | Disc Sequestration
Disc herniations come in three "flavors": disc protrusion (contained herniation or subligamentous herniation), disc extrusion (uncontained herniation or extraligamentous herniation) and disc sequestration.
Although I have created a basic tutorial that covers these three main classes of herniation at the end of the page (The Birth of a Disc Herniation), I shall also discuss them here in a bit more detail.
Disc Protrusion: the nemesis of patients and surgeons alike
 A disc protrusion is a small asymmetric (focal) outpouching of the posterior margin of the disc that occurs because most of the annulus fibrosus has been ruptured by an annular tear, which in turn allows the highly pressurized nucleus pulposus to squeeze through it, only to be barely stopped by these remaining annular fibers. In fact, the pressure of the nuclear material is so great that the disc focally bulges out the end of the annular tear, which is called a disc protrusion.
A disc protrusion is a small asymmetric (focal) outpouching of the posterior margin of the disc that occurs because most of the annulus fibrosus has been ruptured by an annular tear, which in turn allows the highly pressurized nucleus pulposus to squeeze through it, only to be barely stopped by these remaining annular fibers. In fact, the pressure of the nuclear material is so great that the disc focally bulges out the end of the annular tear, which is called a disc protrusion.
Figure 6.1 is a nice example of a small contained disc protrusion that is visualized as a focal asymmetric outpouching of the back of the disc. This herniation is about 4 mm in size and is contacting the left traversing nerve root. Can't see this stuff? If not, then please return to the MRI page for more lessons or click here for more details about figure 6.1.
It is worth repeating the fact that small contained disc herniations are not always associated with back or lower limb pain. Specifically, research has repeatedly demonstrated that small contained disc herniations (a.k.a., protrusions) are seen in approximately 30% of all middle-age people who do not have a history of back or leg pain. [25,75,95,97]
It is also well known that small (less than 5 mm) contained disc herniations have the worst clinical outcomes following discectomy. Specifically, Carragee et al. [22] reported the results of an ingenious study that compared the size of the disc herniation and annular tear, as visualized during the actual surgery, to the two-year post-surgical outcomes. Of the four types of disc herniation/annular tear categories (i.e. fragment-fissure, fragment-defect, fragment-contained, and non-fragment contained), the one composed of small contained disc protrusions had by far the worst improvement with regard to patient pain and disability. (p<0.05)
Therefore, with regard to small disc protrusions, it is best to stick with non-operative care and avoid discectomy unless absolutely necessary. If the patient can't stand the pain and loss of function, then he or she should be worked up for possible fusion as opposed to discectomy.
One possible explanation for this "unwillingness" of contained disc herniations to respond to treatment, may have to do with the bodies inability to naturally reabsorb them. That's right, herniations can be "removed" by the body without surgery. More specifically, several investigations have demonstrated that disc extrusions that have broken through the annulus and posterior longitudinal ligament (PLL) will be reabsorbed (sometimes completely reabsorbed) with the passage of time, [133,135,136] and this reabsorption is positively correlated with clinical outcomes (how good the patient gets after surgery). [135,136] Unfortunately, since the smaller disc protrusions are still contained by the PLL and outer fibers of the annulus, the vessels of the anterior epidural space can't make the contacting needed in order to reabsorb them, which in turn results in a very limited reabsorption and poor recovery. [135,136]
Disc Extrusion: easier for surgeons and the body to handle
 There is no question that if you had to have a disc herniation, a disc extrusion greater than 8 mm in size, with an associated with a narrow annular tear, would be your pick. Not only do these non-contained disc herniations have a better discectomy outcome, [22] they also have a better chance at being naturally reabsorbed by the body which, as we have learned in the last section, has been correlated with good non-operative outcomes. [135-137]
There is no question that if you had to have a disc herniation, a disc extrusion greater than 8 mm in size, with an associated with a narrow annular tear, would be your pick. Not only do these non-contained disc herniations have a better discectomy outcome, [22] they also have a better chance at being naturally reabsorbed by the body which, as we have learned in the last section, has been correlated with good non-operative outcomes. [135-137]
A disc extrusion (figure left) is declared when the contained disc herniation is no longer contained, and the nucleus pulposus has broken through the final layers of the annulus and the posterior longitudinal ligament.
Figure left is a T2-weighted sagittal MRI image that demonstrates a large (9 mm) disc extrusion at L5/S1. Click here to see the sagittal and axial image side-by-side?
{kind=link}
Extrusions are typically bigger than 4-5 mm and can become very large (~18 mm). They also tend to have a more narrow base then disc protrusions and will extend above or below the plane of the disc, which is a key finding in some classification systems.
Typically extrusions, which are rarely seen in asymptomatic people on MRI, [25, 95, 97] may result in lower extremity pain greater than low back pain. Although, I have never found any research on this anecdotal phenomenon, there is perhaps a significant pressure release experience by the posterior annulus when the disc completely ruptures, which in turn reduces some of the pain-generating irritation upon the sinuvertebral nerves in that region.
In an extremely controversial study, Saal et al. [137] published the two-year outcomes of patients who had large CT-confirmed disc extrusions which resulted in unilateral radiculopathy and, in 87% of the cases, significant muscle weakness on examination. Surprisingly, not a single patient in this small group was lost to surgery over the study period and almost half of the patients experienced a greater than 75% reduction in their disc extrusion. In fact, most of the largest disc herniations completely reabsorbed. These findings led the authors to conclude that extrusions can be treated without surgery and natural resolution of the disc extrusion was a common phenomenon. [137] *This very often referenced study must be taken with a grain of salt, for not only was the cohort incredibly small (N = 11) and statistically underpowered, there really was no reported clinical outcomes, other than the fact that none of them were lost to surgery—at least up to the two year time point.
With that admonition, there is decent evidence that demonstrates, again, that these large disc extrusions frequently shrink with the passage of time, [133, 135-137] and this size-reduction is significantly associated with good clinical outcome. [135,136,137]
With regard to surgical success for disc herniation, Carragee et al. [22] reported that disc extrusions which came from a narrow annular tears (fragment-fissure type) were not only the most common type of herniation encountered during surgery, (49% of them) but were also the type that responded the best to discectomy as measured by two-year patient outcomes. Furthermore, disc extrusions of this type had a significantly lower rate (in fact the lowest rate of all disc herniation types) of reoccurrence and subsequent reoperation (1.1%). [22]
Therefore, if the patient has one of these large extrusions and hasn't waited too long (< 1 year at least), then considering microdiscectomy might be a pretty good option if they have failed nonoperative care. *However, if the patient has a large extrusion with an associated wide annular tear (which is quite difficult, if not impossible, to see on MRI), then the surgical outcomes aren't nearly as good, for the rate of disc herniation reoccurrence in these types of herniations has been reported to be as high as 27%, which is completely unacceptable! [22] This is why radiologists really need to describe any visible annular disc tears—especially its magnitude—which they very rarely do! *Yet another reason for you to give me a call :-)
 Okay, at the beginning of this section I promised that I would show you a real example of disc extrusion resorption. Here it is.
Okay, at the beginning of this section I promised that I would show you a real example of disc extrusion resorption. Here it is.
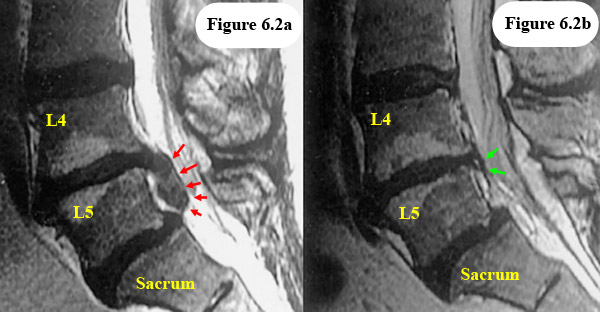
Figure 6.2a demonstrates the initial MRI appearance of a massive disc extrusion (red arrows) which was complete reabsorption (figure 6.2b, green arrows) on the 12-month follow-up MRI. The patient avoided surgery.
Obviously, immediate surgery may be needed if signs of cauda equina syndrome manifest, or if the patient's neurological condition goes downhill, or if the patient simply can't stand the pain any longer; however, other than those indications, the body can has the ability to heal itself.
*Is conservative care really needed? That question has never been addressed in any of these disc extrusion studies, for all patients underwent at least some conservative care. My guess is no, the normal activities of daily living should be enough for most people; I would love to do a study on that to find out for sure.
Why are disc extrusions (and disc sequestrations for that matter) more amenable to natural shrinkage? It is believed that once the herniated nucleus pulposus breaks through the PLL and is thereby exposed to the epidural space, which has a very rich blood supply, neovascularization will occur (blood vessels will grow into the fragment), which in turn results in a wicked inflammatory process. The results of this inflammatory process lead to shrinkage through a macrophage attack of the herniation [134] (the herniation is gobbled up by little Pac-Man like creatures) and dehydration.
Disc Sequestration
A disc sequestration (or a sequestered disc or a disc fragment) occurs when a piece of the disc extrusion breaks loose and moves away to a new location, somewhere within the epidural space.
Figure 6 is an axial view through the disc-level of a motion segment that demonstrates a disc sequestration. Note that the sequestered fragment has broken loose from the main extrusion and compressed the traversing nerve root and thecal sac. You can see a real disc sequestration here.
In reality, as noted during discectomy surgery, very rarely is the fragment completely isolated, for it typically has at least a few fibers still hanging on to the main body.
Compared to the other classes of disc herniation, sequestration is not as frequently seen in patients with low back and/or lower extremity pain.
For example, in 2000, Ahn et al. [135] published the MRI findings of 36 consecutive patients with disc herniations and EMG-confirmed radiculopathy. After agreement by consensus was reached by the study radiologists, it was reported that sequestrations were only seen in 11.1% of the cohort. [135] In a similar but larger study, these results were confirmed by Karppinen et al. when they reported the prevalence of sequestration in 160 patients with sciatica as 8%. [170]
 The figure to the left this from one of my clients who suffered severe left lower extremity pain greater than low back pain following lifting a very heavy object. If you look closely, you can see the orange cutline which is almost down to the L4 disc! This large fragment came from the L3 disc! In other words, the sequestration extends from the L3 to almost the L4 disc!
The figure to the left this from one of my clients who suffered severe left lower extremity pain greater than low back pain following lifting a very heavy object. If you look closely, you can see the orange cutline which is almost down to the L4 disc! This large fragment came from the L3 disc! In other words, the sequestration extends from the L3 to almost the L4 disc!
Although, anecdotally, patients with disc sequestrations are almost immediately referred for spine surgery, a recent 2014 literature review of disc sequestration case reports demonstrated that not all folks do in fact require surgery, as there can be rapid natural sequestration reabsorption, secondary to an inflammatory reaction within the sequestered fragment. [134,135,138]
Histologic studies of sequestered fragments taken at the time of surgery have revealed that they are filled with thin-walled blood vessels and macrophage which were not found in normal age-matched cadaveric disc tissue. [139] Some of these blood vessels were even found growing from epidural fat directly into the sequestration.
One counter intuitive fact about sequestrations is that although they look scary, research has demonstrated that with regard to pain and dysfunction, they are no more painful than either the protrusion or extrusion. [170]
If you do have a patient present with a sequestration, make damn sure that he/she is not having difficulty with bowel or bladder function, or having a progressive loss of motor function, either of which can necessitate an emergency MRI and probably surgery. I would recommend making an early referral to a neurosurgeon or orthopedic surgeon following the discovery of disc sequestration.
Disc Herniation: Evidence-Based Treatment Options:
Spinal Manipulation | Natural Disc Resorption |
 A lumbar disc herniation, which may cause both back and leg pain, should initially be treated with a six-week course of non-operative care (a.k.a., conservative care). [111] However, if there are signs of bowel and bladder dysfunction (cauda equina syndrome); a worsening of neurological symptomatology (especially foot drop); the development of severe unrelenting pain (intractable pain), or a loss of sensation develops in the perineal region, then an immediately spine surgery may be necessary in order to prevent permanent damage.
A lumbar disc herniation, which may cause both back and leg pain, should initially be treated with a six-week course of non-operative care (a.k.a., conservative care). [111] However, if there are signs of bowel and bladder dysfunction (cauda equina syndrome); a worsening of neurological symptomatology (especially foot drop); the development of severe unrelenting pain (intractable pain), or a loss of sensation develops in the perineal region, then an immediately spine surgery may be necessary in order to prevent permanent damage.
Who provides this type of conservative care?
Osteopaths, chiropractors, physical therapists, and acupuncturists are the ones and are typically be the first line of defense against succumbing to surgery. In addition, medical research indicates both over-the-counter and prescription medication should also be considered to to increase the chances of conservative care working.
I will not go through all the different forms of conservative care; however, exercising to tolerance (especially walking over flat ground and, even better yet, swimming) is always an important part of the conservative care treatment package.
DIGRESSION: SPINAL MANIPULATION
 I do have one warning with regard to conservative care and that is about the use of grade 5 manipulation (i.e., cracking the back) as a treatment intervention for back and leg pain caused by a symptomatic lumbar disc herniation or annular tear.
I do have one warning with regard to conservative care and that is about the use of grade 5 manipulation (i.e., cracking the back) as a treatment intervention for back and leg pain caused by a symptomatic lumbar disc herniation or annular tear.
Grade 5 manipulation, which can be performed by osteopaths, chiropractors, and physical therapists, is a by-hand treatment that is typically performed by putting the patient on his or her side (see picture) and then thrusting the doctor's hand into the lumbar spine while tractioning and twisting the spine at the same time.
While such a procedure may be good at correcting back-pain-related facet joint fixations (the joints of the backbones can get stuck and cause pain and even degeneration of that joint), it certainly cannot fix a herniated disc or the annular tear that gave birth to that herniation! On the contrary, it may actually worsen the herniation by ripping open the annular tear (or even widening the tear) which may allow more disc material to spill out and increase the size of the herniation, which in turn may compress the nerve root more and worsen the sciatica.
Manual therapists (i.e., chiropractors, osteopaths, and physical therapists) have been successfully sued for allegedly causing disc herniations or worsening disc herniations to the point it forced their patient into surgery.
In Boucher et al (2014) six successful malpractice cases were described which all involved a chiropractor "allegedly causing or aggravating lumbar disc herniation after spinal manipulative therapy." Among other rulings, the trial judges concluded that "lumbar disc herniations may be triggered by spinal manipulative therapy...."These conclusions were based mainly on expert testimony.
In 2015, Huang et al investigated 10 cases in which chiropractic manipulation was believed to cause a sequestration of the disc (the worst type of herniation). Specifically, all of the patients in the study had a severe increase in low back / leg pain within 24 hours of a chiropractic manipulation and all MRIs performed in the emergency department revealed this sequestrations. They concluded that "spinal manipulative therapy should be prohibited in some large disc herniation patients to prevent neurological damage."
The Finger Cut Analogy:
Let's look at a simple analogy:
 If you had a deep cut along the front of one of your fingers, would you try to stop the finger pain by bending your fingers back in attempts to crack your fingers/knuckles? Maybe the finger pain is coming from a fixation of the metacarpophalangeal joint or one of the interphalangeal joints? It might not be the cut that's causing the pain, it's the fixation of the finger joints... right?
If you had a deep cut along the front of one of your fingers, would you try to stop the finger pain by bending your fingers back in attempts to crack your fingers/knuckles? Maybe the finger pain is coming from a fixation of the metacarpophalangeal joint or one of the interphalangeal joints? It might not be the cut that's causing the pain, it's the fixation of the finger joints... right?
Of course that line of thinking is ridiculous! Not only would the manipulation of a lacerated finger hurt like hell, it would most likely rip out all the scar tissue that the body laid down in efforts to fix the cut. The manipulation may also, if forceful enough, rip the cut open more than it was before.
Therefore, I just don't understand why any healthcare provider would try to treat a symptomatic disc herniation (especially if it is causing mostly sciatica) with a grade 5 "cracking" of the back.
I could go on and on about how the biomechanics of annular tear support my argument, but I think you get the point.
On the other hand, there is a school of chiropractic thought that manipulation is safe (although I still don't know what they're trying to accomplish) which is for supported by some research. I will leave it at that but personally do not recommend any form of grade 5 spinal manipulation for patients with disc herniations-- that is what Cox flexion / distraction treatment was designed for, so why not use that?
Can Any Treatment Reduce the Size of the Disc Herniation without Surgery?
Another warning is this: with the exception of surgical decompression of the disc (discectomy & other surgical procedures), no treatment can reduce the size of a disc herniation. Period, end of story.
I did a search on YouTube the other day for disc herniation repair treatments and was absolutely shocked to see the amount of misleading information and wild claims made by some such as their treatment can heal the disc herniation or suck it back into the disc where it came from. SUCH STATEMENTS ARE COMPLETELY LUDICROUS and unsupported by any type of credible scientific research, whether it be medical or chiropractic.
Distraction Treatments
I have no problem with symptomatic disc herniation patients being treated with distraction methodology. Cox flexion/distraction has been around many years and is reasonably safe and may help prevent spinal surgery.
Although there is not much research to support any type of distraction treatment (Leander, Cox, Vax-D, DRX-9000, etc.), in theory it might have some benefit. I can speculate that it might encourage a diurnal-type effect within the disc which in turn may speed healing.
However, I know of a few patients who have actually been injured with flexion distraction treatment. Specifically, it caused severe sciatica (life-long) in one and particularly. So every treatment has its risks.
Hospitalization for Disc Herniation Related Sciatica: A Very Bad Omen!
It has been known for years that if your disc-herniation-related sciatica is so bad that you require hospitalization, this is a very bad omen for recovery. Specifically, some older studies of the 90s have demonstrated less than one third of such unfortunate patients experience full recovery within one year of that hospitalization. And it didn't matter whether or not these patients had surgical intervention! [152, 153]
In 2017, this topic was revisited by Fjeld et al. These researchers followed 151 consecutive patients that were admitted to the hospital for severe disc-herniation related sciatica to see what happened. They learned a couple of interesting things: #1) if the leg pain was still there at the six-week time point, then it was probably still going to be there at the 12 month time point. the most surprising outcome was the fact that not receiving surgery was actually a bad omen for 12 months! patients with psychosocial issues also did not fare well. [154]
Mother Nature & Natural Disc Herniation Resorption:
Mother nature, on the other hand, via the action of your own bodies immune system, can and does have the ability to reduce the size of the disc herniation with the passage of time, but perhaps not as frequently as we once thought. Let's take a look at the research:
Seo (2014):
In 2014, Seo et al published the results of their investigation which looked that whether or not disc herniations spontaneously reabsorbed and at whether positive herniation resorption was correlated with clinical improvement.
Specifically, 43 patients, all in whom had symptomatic MRI-confirm disc herniations at baseline (the beginning of the study), received six months of conservative care which included meds, PT and epidural steroid injections for those that suffered severe radicular pain. A follow-up MRI was performed at six months to assess the size of the herniation and clinical improvement. What was interesting about this study is that this was the first one to use a novel (new) three-dimensional analysis system which determine the volume of the herniation at baseline and then again in six months.
RESULTS: On average there was a statistically significant (p < 0.01) decrease in the size of the herniation at the six month follow-up. However, not all herniated discs decreased in size (volume). In fact, of the 56 disc herniations looked at, 21 of them (38%) actually increased in size (volume). The authors also discovered, as has been previously demonstrated, [Ahn-1996] that the herniation morphology was predictive of reabsorption. That is, patients with a herniation which disrupted the posterior longitudinal ligament (transligamentous herniations) had a greater chance of resorption. Specifically, 88% of the transligamentous-type demonstrated significant reabsorption, compared with only 42% of patients with subligamentus-type herniations.
This study also looked at clinical outcomes and discovered that at the six month follow-up 14% (6/43) of the cohort actually got worse, conservative care notwithstanding, which forced five of them into emergency discectomy. However, volumetric changes in herniated discs were not significantly related to the clinical outcomes of the patients.Therefore, mechanical compression alone does not explain the symptoms of lumbar disc herniation. Other factors must be involved, such as chemical irritation. [26-29] They concluded by saying, "in contrast to prior studies, we found that lumbar disc herniation is a dynamic disease that does not always resolves spontaneously."
So it is not the magical treatment of the practitioner that reduces the size of some disc herniations in some cases, but the incredible intelligence of your own body.
Conservative care, which typically consists of rest, medication, physical therapy, bracing, exercise, low-force chiropractic care and acupuncture, is usually quite effective at helping the natural recovery process [126] and only fails in about 1-2% of the people who try it. [8,9,105] However, recovery from a severely symptomatic disc herniation may take years, and some patients never completely recover. [22,74]
Okay, I can hear you saying "How do you know recovery is slow and potentially never complete? Notwithstanding my own personal experience with discectomy and chronic pain, the award-winning Weber study [74] demonstrated that approximately 19% of the cohort (the group of people being studied) had continued low back pain even 10 years after the start of the study, regardless of whether they underwent discectomy or non-surgical treatment for their disc herniation. [74]
Psychotherapy may also be helpful for the situational depression that often develops because of the chronic pain and loss of function associated with lumbar disc herniation.
Although there is going to be some overlap, the treatment for symptomatic disc herniation can be slightly different depending on whether or not the symptoms are mainly low back pain versus mainly lower limb pain. Let's talk about them one at a time.
Cribb et al (2007):
In this study, which was published in the prestigious Journal of Bone & Joint Surgery (Br), 15 patients with "massive" disc herniations were followed for an average of two years to see what happened to them. They all had a disc herniation which was causing severe radicular pain (leg pain/sciatica). Decompressive surgery (microdiscectomy) was recommended for all of them in fear of cauda equina syndrome development. At an average two-year follow-up, it was discovered that none of the developed cauda equina syndrome and all of those disc herniations significantly decreased in size. Specifically, the average herniation resorption was 80% (range: 68% to 100%).
The Bottom Line: with regard to waiting around for mother nature, she will, in most cases, naturally decrease the size of the disc herniation but usually only if that herniation is large. She does not do very well with decreasing the size of disc bulges or contain disc herniations. This is because the small herniation fragment is still out-of-sight of the body's immune system and therefore a macrophage attack cannot begin.
However, it is also known that in order to increase your chances of reversing motor loss (muscle damage) from a disc herniation, you don't want to wait more than three or four months to have that nerve surgically freed up in the herniation removed.
A Little Advertisement: unless your objective findings and/or symptoms put you in the absolute indication for spine surgery category, which doesn't happen that often, it can be very difficult deciding whether or not to try such a procedure. Why not let me help you with that decision, like thousands already have: if you're interested, please check out Dr. Gillard's Coaching Service
Disc Herniation Related Low-Back Pain: Treatment Via Experimental Procedures?
If conservative care fails, the next tier of treatment for disc-herniation-related low-back pain does not have a very good track record. [74,110] Specifically, as demonstrated by Chou in 2009, [110] these treatment interventions, which include SED, Nucleoplasty, PIRFT, RF-Denervation, Spinal Cord Stimulator, IDET, Prolotherapy, and Intradiscal Injection, continue to be unsupported by high-quality scientific research, which is virtually nonexistent. Therefore, until more high-quality research is performed, I would not suggest trying any of these experimental treatments at this time (2014). [110] Why? Because there is strong evidence, from both animal and human research, that poking a hole in the disc—a requirement for many of these treatments—is not a good thing, and will lead to future degeneration, annular tears, and even disc herniations. [Footnote]
However, there is one procedure in this group that might be worth keeping an eye on.
Intradiscal Biacuplasty
In a recent well-designed investigation, researchers demonstrated that intradiscal biacuplasty, which is a minimally invasive procedure that uses radiofrequency energy to treat the annular tear component of the disc herniation, was superior (P<0.05) to a sham (fake) biacuplasty procedure for the treatment of chronic disc-herniation-related low-back pain. [120]
 Specifically, Kapural et al. [120] reported the six-month results of their randomized, placebo-controlled trial (this type of design produces very high quality scientific evidence) that randomly (the patient got assigned to a group by luck of the draw) placed 64 chronic-pain-suffering patients (all of whom were diagnosed with lumbar discogenic pain) into either a real or fake biacuplasty treatment group.
Specifically, Kapural et al. [120] reported the six-month results of their randomized, placebo-controlled trial (this type of design produces very high quality scientific evidence) that randomly (the patient got assigned to a group by luck of the draw) placed 64 chronic-pain-suffering patients (all of whom were diagnosed with lumbar discogenic pain) into either a real or fake biacuplasty treatment group.
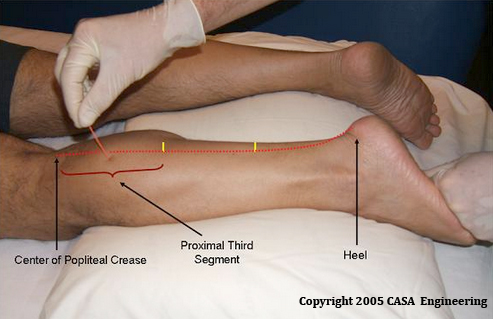
The fake biacuplasty procedure put the patient through the same preoperative and operative steps as the real biacuplasty procedure, which included poking the cannulas through the muscles of the low back. (figure 7.5) However, the machine that generated the RF current (this current is used to cauterize the annular tear closed) was rigged so that no current was flowing. In other words, the machine was not working.
The beauty of this study design was that neither the patients nor the patient's treating doctors knew whether or not the real biacuplasty have been performed (this is called blinding) until after the six-month evaluation.
At the six-month evaluation, patients from the real biacuplasty group reported a significant (p<0.05) decrease in their pain and increase in their ability to function, as compared to patients in the fake biacuplasty group. [120]
Part two of this investigation is now underway. Not only will clinical outcomes being checked again further on down the road, patients in the fake biacuplasty group were allowed to cross over (have the real procedure) and will be followed.
I eagerly await the results of their next evaluation and be sure to keep my readers updated and is most fascinating study. Will the original biacuplasty group keep that advantage with regard to outcomes? Will the crossover patients also achieve significant improvement from the real procedure? We will just have to wait and see.
*I want to publicly congratulate Kapural and his team of investigators for daring to put one of these experimental treatments through a "real" scientific study and strongly urge the patent-holders on IDET, SED, Nucleoplasty, discTRODE, and PIRFT, to begin their own studies with this same design, for until they do, I will not be able to recommend these procedures for the treatment of chronic back and/or leg pain.
Epidural Steroid Injections For Disc-Herniation-Related Low Back Pain
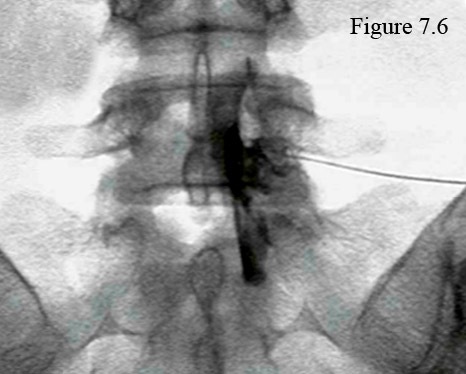 Although epidural steroid injections (ESIs) are typically thought of as a treatment for the radicular pain associated with disc herniation, there is significant medical evidence that demonstrates ESIs can also be used to reduce the low-back pain associated with disc herniation. [109,110,123,130- 132]
Although epidural steroid injections (ESIs) are typically thought of as a treatment for the radicular pain associated with disc herniation, there is significant medical evidence that demonstrates ESIs can also be used to reduce the low-back pain associated with disc herniation. [109,110,123,130- 132]
Figure 7.6 is an anterior-posterior fluoroscopic image taken after the contrast injection during a transforaminal ESI procedure, done for a symptomatic L5/S1 disc herniation. Note the nearly-horizontal needle positioned within the right neural foramen and the outline of the contrast (black) which has diffuse down to cover the L5/S1 herniation region as well as the S1 traversing root. (Click here if you're having trouble seeing this.)
What is an epidural steroid injection? In a nutshell, an ESI, which have been around since the 1950s, is an outpatient medical procedure that involves inserting a thin needle into the epidural space at the level of the disc herniation and then injecting a corticosteroid (a very powerful anti-inflammatory) and anesthetic, which in turn travels from the injection site to the symptomatic disc herniation and reduces the pain-generating inflammatory process.
Who should perform the ESI procedure? Although many doctors of many different specialties are doing these procedures in this day and age of post-Obama care, only a fellowship-trained interventional pain medicine physician—one who has devoted his entire practice to using these injective procedures—would be good enough to treat my patients or me. [123]
Do epidural steroids really work? Unlike the experimental procedures mentioned above, there has been a lot of research performed on epidural steroid injections, and the short answer is yes, they do work in the short term (< 6months) for the relief of back and leg pain associated with disc herniation. [110,125] However, if you have spondylolisthesis or have waited longer than a year to try them, then the chances of success are not as good. [125] It is, however, important to understand that there's no significant evidence that demonstrates ESIs will have any effect on long-term clinical outcomes. [110] In other words, they are not going to affect how you are doing five years after the herniation occurs.
 Another very important component of the ESI procedure is fluoroscopic imaging. Specifically, the fluoroscopy procedure uses a special low-radiation x-ray machine (figure 8) that creates a continuous radiographic picture (kind of like the one created when you pass through security screening at the airport) of the low back during the procedure. This way the physician can see exactly where the tip of the razor-sharp needle is at all times, which not only increases the chances of proper placement of the injectate (steroid + anesthetic), [127] but decreases the chances of patient injury. [124] Fluoroscopic guidance should be used during all ESI procedures, no matter which of the three approaches is used. [125]
Another very important component of the ESI procedure is fluoroscopic imaging. Specifically, the fluoroscopy procedure uses a special low-radiation x-ray machine (figure 8) that creates a continuous radiographic picture (kind of like the one created when you pass through security screening at the airport) of the low back during the procedure. This way the physician can see exactly where the tip of the razor-sharp needle is at all times, which not only increases the chances of proper placement of the injectate (steroid + anesthetic), [127] but decreases the chances of patient injury. [124] Fluoroscopic guidance should be used during all ESI procedures, no matter which of the three approaches is used. [125]
Although using fluoroscopy during the procedure may sound like a no-brainer, you would be shocked at the number of physicians who don't use it, which results in the steroid being injected into the wrong spot 30-40% of the time! [125,127] Furthermore, by not using fluoroscopic guidance (or CT guidance) the risk of minor and major procedural complications significantly rises. [124] Therefore, I would not allow any of my patients or myself to undergo ESI without it.
The final things to understand about ESIs is that in order to get the desired effect (decrease in back and/or leg pain), you will most likely have to undergo more than one procedure. However, you should not have more than three ESIs per year;[123] although, if the first ESI fails to reduce your pain, then a second ESI will probably fail as well, and really shouldn't be attempted. [113]
As noted above, the ESI procedure can be done via three different approaches. Let's talk about them.
Caudal ESIs involve threading the needle completely through the narrow caudal canal of the sacrum and then releasing the steroid into the posterior epidural space (which of course is behind the thecal sac) only at the level of L5/S1. After its release the injectate (steroid + numbing-agent) must diffuse from the posterior epidural space, around the thecal sac, and (hopefully) enter the anterior epidural space in order to find its target (the disc herniation). Although this technique is still useful for patients who have suffered a lot of scar tissue (perineural fibrosis) in the anterior epidural space from a previous spine surgery, the technique has really fallen out of favor and is not encouraged. [123, 125]
Interlaminar ESIs, which are still commonly used today, involve putting the needle between the lamina of the affected motion segment and then through the ligamentum flavum, which results in a "pop" and "loss of resistance" that the injectionist (doctor doing the procedure) can hear and feel. Like the caudal ESI, the injectate is released into the posterior epidural space and has to migrate around the thecal sac to the anterior epidural space in order to find its target. Again, some authors believe it "improbable" that the steroid will actually reach its target in the anterior epidural space and discourage the use of this procedure. [125]
 Transforaminal ESIs, which are very popular these days, involve placing the needle within the neural foramen of the affected motion segment, after which the steroid is released into the foramen and distal anterior epidural space. The injectate now must travel only a short distance to reach the disc herniation target. (figure 7.6 & 7.9)
Transforaminal ESIs, which are very popular these days, involve placing the needle within the neural foramen of the affected motion segment, after which the steroid is released into the foramen and distal anterior epidural space. The injectate now must travel only a short distance to reach the disc herniation target. (figure 7.6 & 7.9)
Figure 7.9 is a para-sagittal cartoon through the neural foramina that demonstrates the traditional needle placement for a transforaminal ESI.
Note the good-sized vein that is in close proximity to the needle tip. Now, perhaps you may realize why using fluoroscopic guidance is so important when performing ESIs. Even with the use of fluoroscopy, there is vascular penetration of the needle tip into the vein 7.4% of the time. [124] Luckily, because of the fluoroscopic guidance, the injectionist will soon realize that he has "poked" the vein and will reposition the needle accordingly.
Because of the long distance between the site of injection and the disc herniation target, both interlaminar and caudal ESIs must use a significantly higher volume of steroid (typically ~9mL) in order to be effective. [130,132] Such a high volume of steroid can increase the risk for large spikes in blood glucose and blood pressure, which might not bode well for patients who are diabetic and/or hypertensive. On the other hand, because they are performed within the anterior epidural space, transforaminal ESIs use a much lower volume of steroid (typically ~3mL) yet are just as effective, if not more effective then the posterior epidural procedures. [131]
Personally, I have had both the interlaminar and transforaminal injections and, although they both eliminated back and leg pain, the transforaminal effect lasted much longer (one month) than the interlaminar injection (one week).
Fusion For Disc-Herniation-Related Low Back Pain
If the patient simply can't stand the low back pain and loss of function associated with disc herniation (I would expect their Oswestry Disability Index (ODI) score to be >48%), and if they have failed non-operative care, then, and only then, should they consider lumbar interbody fusion. [111] Personally, I believe 18 months of conservative care should be exhausted before going down the road of fusion.
Lumbar interbody fusion, which is a very invasive (destructive) procedure, typically involves the surgical removal of the disc herniation, annular tear and entire nucleus pulposus, which in turn is thought to eliminate the sources of chronic back and leg pain associated with disc herniation. Next, an interbody spacer (commonly called a cage) will be inserted into the empty center of the disc, thereby reestablishing axial load through the center of the motion segment. Then, through the use of pedicle screws and rods, the proper sagittal alignment of the motion segment will be restored.
Once the proper alignment has been achieved, the two vertebrae will be permanently "fused" into that position by taking bone from the patient's own hip (iliac crest autograft) and then packing it into the remaining disc space, and between the decorticated (roughened up and bleeding) transverse processes, facets, and laminae. This iliac crest autograft may be thought of as the "glue" that will hold the motion segment permanently together in the proper position but as one unit, thereby eliminating any pain-generating movement between the vertebrae.
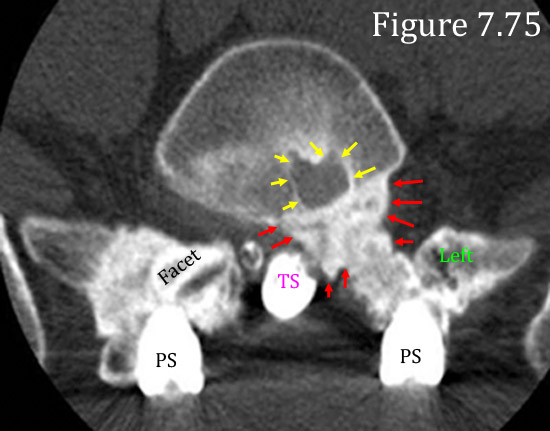 The time-to-fuse (i.e., the time needed for the hip bone to harden and unite the two vertebrae into one unit) is typically about 12 months, unless you are brave enough to use recombinant human bone morphogenetic protein-2 (rH-BMP-2).
The time-to-fuse (i.e., the time needed for the hip bone to harden and unite the two vertebrae into one unit) is typically about 12 months, unless you are brave enough to use recombinant human bone morphogenetic protein-2 (rH-BMP-2).
Figure 7.75 is an axial CT image through the L5/S1 disc space which has been affected by severe rH-BMP-2-related complications. The yellow arrows are pointing to a hole in the L5 vertebral body (osteolysis) and the red arrows are pointing to a massive growth of extra bone formation that has migrated from the surgical site into the lateral recess. This patient had severe left lower extremity pain after fusion and needed a decompressive second surgery for removal of this bone.
Although rH-BMP-2 may cut the time-to-fuse in half, as well increase the rate of successful fusion to near 100% (*remember, just because the fusion is successful {i.e., the hip bone hardens the motion segment into one unit}, doesn't mean the back and/or leg pain will go away), there is about a 30% chance that you will develop typically-minor complications from its use and and ~3% chance for severe complications. [Personal knowledge] Furthermore, rH-BMP-2 might be related to the development of cancer. [121, 122] Therefore, until rH-BMP-2 is further studied, I would not suggest using it unless you are at high risk for failure-to-fuse, and even then you must carefully weigh the risks versus rewards. (See the Fusion Page for more information.)
Disc Herniation Related Lower-Limb Pain: How Is Sciatica Treated?
Again, conservative care is always the first line of defense and should be tried for at least six weeks before moving on to the more invasive procedures like epidural steroid injections (ESIs). Please review the start of this section for more information on conservative care.
Epidural Steroid Injections
For patients who were refractory (didn't respond well) to nonoperative care, a trial of epidural steroid injections (ESIs) may be advisable at this point. [110,111] Please refer to the epidural steroid section above, which covers ESIs for the treatment of both back and radicular pain related to disc herniation.
Disc Herniation: Surgical Options
When conservative care and epidural steroid injections have failed, and the patient can no longer take the excruciating lower extremity pain associated with disc herniation, then it is time to consider surgical intervention, which is needed in about 0.05-0.005% of the population [8,9], or in about 1.7% of patients who were hospitalized from the pain of disc herniation. [93]
A surgery called discectomy, which can be performed via a microscope or loupe magnification, or even openly, is a well-researched treatment intervention for symptomatic disc herniations that are causing lower limb pain (akas: leg pain, lower extremity pain, sciatica, radicular pain) greater than low back pain. [74,81]
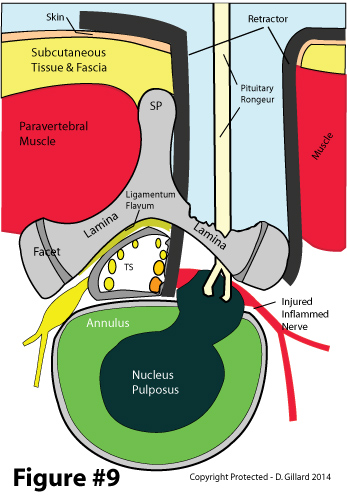 Of all the available types of spine surgery, discectomy is often believed to be the most effective if, let me repeat that, if, you are a proper candidate for the procedure. What is a proper candidate? Well, the ideal candidate would be a patient with complaints of 80% radicular pain, 20% low back pain; a positive MRI that demonstrates a single-level compressive disc extrusion greater than 7 mm in size and with a narrow annular channel; [22] a positive EMG/NCV that demonstrates radiculopathy at the same level as the herniation; and examination findings that include a positive straight leg raise and neurological findings that match the MRI and EMG.
Of all the available types of spine surgery, discectomy is often believed to be the most effective if, let me repeat that, if, you are a proper candidate for the procedure. What is a proper candidate? Well, the ideal candidate would be a patient with complaints of 80% radicular pain, 20% low back pain; a positive MRI that demonstrates a single-level compressive disc extrusion greater than 7 mm in size and with a narrow annular channel; [22] a positive EMG/NCV that demonstrates radiculopathy at the same level as the herniation; and examination findings that include a positive straight leg raise and neurological findings that match the MRI and EMG.
In a nutshell, as depicted in figure 9, the discectomy procedure begins with the surgeon cutting through the back muscles and then exposing the laminae at the level of herniation. Usually a little of the superior and inferior lamina will need to be removed (this is called a laminotomy) in order to create a big enough window to operate through. Once the window was created, ligamentum flavum is removed and the thecal sac and/or traversing nerve root is retracted medially, in order to to visualize a central or paracentral disc herniation. Finally, the herniation is removed and the surgical wound closed.
The topic of discectomy is so large, that I have devoted an entire page to it. Please visit the Discectomy Page for more information.
Well that pretty much does it for the new and improved disc herniation page, which was created during the month of April and May, 2014.
I shall leave this old tutorial here that is still a good read and has been very popular over the years.
The Birth of a Disc Herniation
Lets begin our tutorial with a quick review of the normal disc and then proceed through each type of herniation.
The Normal Disc:
Figure #1: The nucleus pulposus (pink #1) is the proteoglycans-rich substance in the center of the disc that has the job of transmitting the axial load of the body and gravity from the center of one vertebra to the center of the next vertebra. It also acts as a pivot-point at which all trunk motion occurs. Under normal conditions, the nucleus is tightly held in place by the cartilaginous annulus fibrosus, (green #2) which is made from strong concentric rings of type I collagen called lamellae (#9). It is this specially arranged collagen that gives the annulus the tremendous strength needed to hold that nucleus in place, which is under constant axial load.
Key Concept: because of the constant axial load up on it, the nucleus pulposus is always trying to escape (or squirt out) from its annular confines, which happen to be weaker in the posterior region of the disc. Also noteworthy is the fact that the posterior one third of the annulus is innervated (has nerves in it) by the sinuvertebral nerve (SN) and is quite capable of transmitting signals of pain from the disc to the brain.
The Disc Bulge: The First Step Towards Disc Herniation
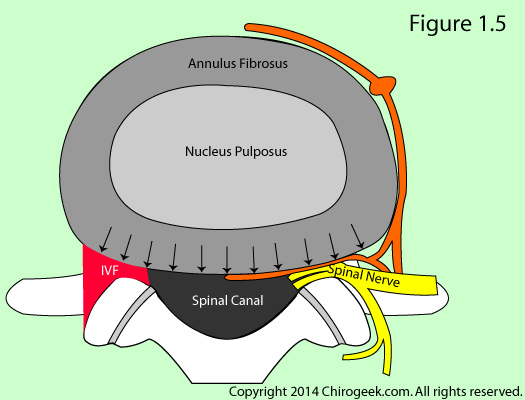 In order for a disc to herniate, its structural components must first tear and/or weaken. This weakening is thought to result from a condition called Degenerative Disc Disease (DDD). Although all human discs undergo a natural aging process, some suffer an accelerated aging process that may occur from genetic predisposition, injury to the disc, or participating in strenuous work activities.
In order for a disc to herniate, its structural components must first tear and/or weaken. This weakening is thought to result from a condition called Degenerative Disc Disease (DDD). Although all human discs undergo a natural aging process, some suffer an accelerated aging process that may occur from genetic predisposition, injury to the disc, or participating in strenuous work activities.
Regardless of the cause, DDD weakens the lamellae of the annulus and allow them to "bulge" backwards, which in turn allows the posterior of the disc to symmetrically bulge out (black arrows figure 1.5), which may or may not be associated with annular tearing.
This condition, which can be seen in 60-80% of middle-page people without backward leg pain, [75,97] is called a disc bulge and is typically not a cause of low back pain; that is, unless it is harboring an annular tear.
The Annular Tear: The Second Step Towards Disc Herniation
 Because the lamellae of the annulus are often incomplete in the posterior region of the disc, occasionally the nucleus can break through the annulus which results in an annular tear.
Because the lamellae of the annulus are often incomplete in the posterior region of the disc, occasionally the nucleus can break through the annulus which results in an annular tear.
Only annular tears that reach the outer one third of the annulus (figure 2) which is innervated by nociceptive fiber from the sinuvertebral nerve have the ability to generate low back pain. These types of tears, which are called full thickness or grade III annular tears, not only destroy the normal biomechanics of the disc, the physical contact by nucleus pulposus upon the nerve fiber may result in a pain-generating inflammatory process. (Read more about Annular Tears)
Key Concept: a pain-generating full thickness annular tear is usually completely hidden within a bulging disc on MRI and is only visible on a test called provocative discography, which you don't want to do unless you are ready to have fusion. (Read more about Provocative Discography) It is also important to understand that a disc herniation is not possible (there are rare exceptions) without the annular tear.
The Disc Protrusion: The First Class of Disc Herniation Is Born
 When the outer fibers of the annulus and posterior longitudinal ligament (PLL) have almost completely ruptured through, you often get an asymmetric or focal outpouching in the posterior disc which is called a disc protrusion (a.k.a., contained disc herniation), which is demonstrated quite nicely on figure 3.
When the outer fibers of the annulus and posterior longitudinal ligament (PLL) have almost completely ruptured through, you often get an asymmetric or focal outpouching in the posterior disc which is called a disc protrusion (a.k.a., contained disc herniation), which is demonstrated quite nicely on figure 3.
Disc protrusions, which are typically ~4mm in size, usually cause lower back pain symptoms greater than lower limb symptoms and are very difficult to treat.
The reason for more low back pain is because a pressure can build up in the posterior one third of the disc (the PLL and outer annulus is still intact) which mechanically irritates the already inflamed nociceptors of the sinuvertebral nerve.
Key Concept: The contained disc herniation is not always symptomatic and shows up on MRI in about 30% of middle-age people without back or leg pain. [25] Furthermore, if they are symptomatic, they have a very poor track record with regard to surgery (microdiscectomy), especially if less than 8 mm in size. [22] So be very careful if a spine surgeon wants to operate on your 4 mm contained herniation! (*I wish that I would would have known this fact before I had my failed microdiscectomy.)
The Disc Extrusion: The Second Class of Disc Herniation
 When the final layers of the annulus and PLL completely rupture, the herniated portion of nucleus pulposus can become quite large and cause severe lower limb pain (sciatica or radicular pain), which is typically greater than low back pain.
When the final layers of the annulus and PLL completely rupture, the herniated portion of nucleus pulposus can become quite large and cause severe lower limb pain (sciatica or radicular pain), which is typically greater than low back pain.
This type of herniation is called a disc extrusion (a.k.a., non-contain disc herniation) and is not typically seen on MRI in asymptomatic people. [25,95,97]
In figure 4, note that the PLL (blue) has completely ruptured and resulted in the creation of a 10 mm extrusion, which is compressing both the traversing (white star) and exiting (green star) nerve roots.
Since a lot of the pressure has been relieved in the posterior annulus because of the rupture, anecdotally (I've never seen a study on this, but it would make a great one) patients have diminished low back pain, but significantly worsened lower limb pain.
Unlike small contain disc herniations, disc extrusions typically respond very well to microdiscectomy if the size of the annular tear is not too large (there's no way to tell this except at the time of surgery) and if the patient has not waited too long (more than a year) to have the surgery. [22]
Another interesting fact about these large disc extrusions is that the body has a pretty good track record for naturally reabsorbing them (making them disappear). In fact, research has demonstrated that 80% of large disc extrusions will naturally decrease in size by 50% within one year. [5,6] Unfortunately, since the ideal timing of surgery for these herniations is ~4 months, the damage may already be done if you wait for this natural process to occur.
The Disc Sequestration: The Final Class of the Disc Herniation
 Sometimes a piece of extruded disc material (blue star) can break loose from the main body of the extrusion and freely move within the epidural space.
Sometimes a piece of extruded disc material (blue star) can break loose from the main body of the extrusion and freely move within the epidural space.
This type of herniation is called a sequestration and (to my knowledge) has never been seen in asymptomatic people on MRI. [25,75,95,97]
Although some research has demonstrated that the sequestration is not more painful than an extrusion or even contained herniation, [23] if the fragment is large enough, there is concern that it may cause severe compression on the cauda equina, which in turn may lead to bowel and/or bladder control (the patient may lose control of the ability to pee and poop), which is considered a medical emergency, and is called the cauda equina syndrome.
Any patients who develop such symptomatology, must immediately present to the emergency room for evaluation, because waiting too long may result in permanent damage to the nerves that control your bowel/bladder function.
REFERENCES
1) Milette PC, et al. “Radiating Pain to the Lower Extremities Caused by Lumbar Disk Rupture without Spinal Nerve Root Involvement.” AJNR Am J Neuroradiol 1995; 16:1605-1613
2) Ohnmeiss DD, et al "Degree of disc disruption and lower extremity pain" Spine - 1997; 22(14):1600-1665 (also in several other journals in 1999)
3) Marshall LL, et al. “Chemical irritation of nerve root in disc prolapse.” Lancet 1973; 2:320
4) Marshall LL, et al. “Chemical Radiculitis: A clinical, physiological and immunological study. Clin Orthop 129:61-67, 1977
5) Saal JA, Saal JS, Richard JH. The natural history of lumbar intervertebral disc extrusion treated nonoperatively. Spine
1990,15:683–6.
6) Eiichi Takada and Masaya Takahashi et al. "Natural history of lumbar disc hernia with radicular leg pain: Spontaneous MRI changes of the herniated mass and correlation with clinical outcome. "Journal of Orthopaedic Surgery 2001, 9(1): 1–7.
7) Goupille et al. "Percutaneous Laser Disc Decompression for the treatment of Lumbar disc herniation." Semin Arthritis Rheum. 2007 Mar 13; (Epub ahead of print).
8) Anderson GBJ. The Epidemiology of Spinal Disorders. In: Frymoyer JW, ed. The Adult Spin. New York: Raven press; 1997
9) Van de Velden J, de Bakker DH. Basisrapport: morbiditeit in de huisartsenpraktijk. Utrecht: Nivel;1990
10) Carragee EJ, et al. "Can MR scanning in patients with sciatica predict failure of open limited discectomy? Proceedings of the international Society for the study of lumbar spine (ISSLS) Scotland, June 2001.
11) Peng B, Wenwen W, et al. “Chemical Radiculitis." (2007) Pain 127(11-16)
12) Andersson GB, Herkowitz HN, Katz JN. Indications for thoracic and lumbar spine fusion and trends in use. Orthop Clin North Am 1998; 29:803.
13) Atlas SJ, Keller RB, Deyo RA, Singer DE. Long-term outcomes of surgical and nonsurgical management of sciatica secondary to a lumbar disc herniation: 10 year results from the Maine lumbar spine study. Spine 2005; 30:927-935. [Read my review]
14) Brouwer PA, et al. "effectiveness of percutaneous laser disc decompression versus conventional open discectomy in the treatment of lumbar disc herniation; design of a prospective randomized controlled trial." 2009; BMC Musculoskeletal Disorders 10:49
15) Schenk B, et al (2006) Percutaneous Laser Discectomy: A Review of the Literature. AJNR; January 2006: 27; 232-235 [here]
16) Singh V, et al "Percutaneous Disc Decompression using coblation (Nucleoplasty) In the Treatment of Chronic Discogenic Pain." 2002 Pain Physician, Volume 5, Number 3, pp 250-259 ASIPP.
17) Waddell G. "A new clinical model for the treatment of low back pain." (1987) Spine; 12:632-44
18) Croft PR et al. "Outcome of low back pain in general practice prospective study." (1998) BMJ; 316:1356-9.
19) Schwarzer AC, Aprill CN, Derby R, Bogduk N, Kine G. "The prevalence and clinical features of internal distant instruction in patients with chronic low back pain." (1995) Spine; 20(17):1878-83.
20) Manninen P, et al. "Incidence and risk factors of low-back pain in middle aged farmers." (1995) Occupation Med (Oxf; 45:141-146)
21) Merskey H, Bogduk N. “Classification of Chronic Pain: Descriptions of Chronic Pain Syndromes and Definitions of Pain Terms.” Seattle: IASP Press, 1994:180-1
22) Carragee EJ, et al "Clinical outcomes after lumbar discectomy for sciatica: The effects of fragment types and annular competence" J Bone Joint Surg Am - 2003; 85(1):102-108
23) Karppinen J. et al. “Severity of Symptoms and Signs in Relation to Magnetic Resonance Imaging Findings Among Sciatic Patients.” Spine 2001 ;26(7):E149-E154 [here's my review].
24) Modic MT, et al. “Contrast-enhanced MR imaging in acute lumbar radiculopathy: a pilot study of the natural history.” Radiology 1995 ;195:429-35
25) Jensen MC, et al. “MRI imaging of the lumbar spine in people without back pain.” N Engl J Med – 1994; 331:369-373.
26) Boden SD et al. “Abnormal magnetic resonance scans of the lumbar spine in asymptomatic subjects: A prospective investigation.” J Bone Joint Surg Am 1990; 72A:403-408
27) Lawrence RC, et al. "estimates of the prevalence of arthritis and selected musculoskeletal disorders in the United States." (1998) Arthritis Rheum; 41:778-799.
28) Gureje O, et al. "Persistent pain and well-being: a World Health Organization study of primary care." (1998); 280:147-151
29) Cassidy D, et al. "The Scandinavian health and back pain survey." (1998); 23:1860-67
30) Manchikanti L. "Epidemiology of Low Back Pain." (2000); 3:167-192
31) Walker BF. "The Prevalence of Low Back Pain: (2000); J Spinal Discord; (13:205-217
32) Kuslich SD, Ulstrom CL, Michael CJ. "The Tissue Origin of Low Back Pain and Sciatica: A report of pain response to tissue stimulation during operations on the lumbar spine using local anesthesia." Orthop Clinics North Am 1991;22:181-187.
33) Manchikanti L, Derby R, Hirsch JA, et al. "a systematic review of mechanical disc decompression with nucleoplasty." Pain Physician 2009; 12:561-572
34) Chen YC et al. "intradiscal pressure study of percutaneous disc decompression with nucleoplasty in human cadavers." Spine 2003; 28:661-665.
35) Kambin P, et al. "percutaneous posterolateral discectomy. Anatomy and mechanism." Clin Orthop Relat Res 1987; 223:145-154.
36) Kambin P, el al. "Percutaneous lumbar discectomy. Review of 100 patients and current practice." Clin Orthop Relat Res 1989: 238:24-34
37) Karasek M, Bogduk N. "12 month follow-up of controlled trial of intradiscal thermal annuloplasty (IDET) four back pain do to internal disc disruption." spine 2000; 25:2601-2607.
38) Nerubay J, et al. "percutaneous laser nucleolysis of the intervertebral disc. An experimental study." Clin Orthop Relat Res 1997; 337:42-44.
39) Sasaki M, et al. "effects of chondroitinase ACB on intradiscal pressure in sheep: an invivo study." Spine 2001; 26:463-468.
40) Gibson JNA, Waddell G. "surgical interventions for lumbar disc prolapse." Cochrane Database Syst Rev 2009; 1:CD001350.
41) Chen YC, et al. "intradiscal pressure study of percutaneous disc decompression with nucleoplasty in human cadavers." Spine 2003; 28:661-665.
42) Mixter W, Barr J. rupture of the intervertebral disc with involvement of the spinal canal." N Engl J Med 1934; 211:210-215.
43) Smith L. "enzymatic dissolution of the nucleus pulposus in humans." JAMA 1964; 187:137-140.
44) Hijikata S. "percutaneous Nucleotomy: a method of percutaneous nuclear extraction." J Toden Hospital 1975; 5:39-44.
45) Onik G, et al. "percutaneous lumbar discectomy using a new aspiration probe." AJNR 1985; 6:290-293.
46) Derby R, Baker RM, Lee CH. "evidence-informed management of chronic low back pain with minimally invasive nuclear decompression." Spine J 2008;8:150-159
47) Chen YC, et al. "histologic findings of disc, end-plate and neural elements after a collation of nucleus pulposus: an experimental nucleoplasty study." Spine J 2003; 3:466-470.
48) Phurrough S, et al. "Decision Memo for Thermal Intradiscal Procedures. 2008 [cited September 30, 2008]. www.cms.hhs.gov/mcd/viewdecisionmemo.asp?from2=viewdecisionmemo.asp&id=215&
50) Ng LC, Sell P. 'Predictive value of the duration of sciatica for lumbar discectomy. A prospective cohort study.'J Bone Joint Surg Br. 2004 May;86(4):546-9 " Patients with an uncontained herniated disc had a shorter duration of symptoms and a better functional outcome than those with a contained herniation."
51) Dewing CB, et al. "the outcome of lumbar microdiscectomy in a young, active population: correlation by herniation type and level." Spine 2008; 33:33-38.
52) Rheinhard SWR, Kraemer J. "chemonucleolysis versus laser disk decompression: a prospective randomized trial." Bone Joint Surg Br 1997; 79:247.
53) Spitzer WO, LeBlanc FE, DuPuis M. "Scientific approach to the assessment and management of activity-related spine disorders: a monograph for clinicians. Spine 1987; 12 (supplemental): 55-59.
54) Walker BF, Muller R, Grant WD. Low Back Pain in Australian Adults. Prevalence And Associated Disability. J Manip Physiio Ther 27 (4): 238-244.
55) Jeffries LJ, Milanese SF, Grimmer-Somers KA. Epidemiology of Adolescent Spine Pain. A Systematic Overview of the Research Literature. Spine 32 (23): 2630-2637.
56) Clinical Standards Advisory Group. Epidemiology Review: The Epidemiology and Cost of Back Pain. London: HMSO, 1994:1.
57) Vingard E, Mortimer M, Wiktorin C, et al. Seeking Care for Low Back Pain in the General Population: A Two-Year Follow-Up Study: results from the MUSIC-Norrtalje study. Spine 2002; 27 (19): 2159-2165.
58) Carey TS, Garrett JM, Jackman AM. Beyond the good prognosis: examination of an inception cohort of patients with chronic low back pain. Spine 2000; 25:115-120.*
59 ) Croft PR, Macfarlane GJ, Papageorgiou AC, et al. Outcome of Low Back Pain in a general practice: A prospective study. BMJ 1998; 316:1356-1359.
60 Hagen KB, Thune O. Work in capacity from low back pain in the general population. Spine 1998; 23:2091-2095.
61) von Korff M. Studying the natural history of back pain. Spine 1994; 19:2041-2046.
62) Seferlis T, Nemeth G, Carlsson A-M. Prediction of Functional Disability, recurrences, and chronicity after one year and 180 patients sick-listed for acute low back pain.* J Spinal Disord 2000; 13:470-477.
63) Deyo RA, Tsui-Wu YJ. Descriptive Epidemiology of Low Back Pain And Its Related Medical Care in the United States. Spine 1987; 12:264-268.*
64) Rhee JM, Schaufele M, Abdu WA. Radiculopathy and the Herniated Disc. Controversies regarding pathophysiology and management. J Bone Joint Surg Am. 2006; 88:2070-2080.*
65) Boden SD, Davis DO, Dina TS, et al. Abnormal Magnetic Resonance Scans of the Lumbar Spine in Asymptomatic Subjects a prospective investigation. J Bone Joint Surg Am. 1990; 72:403-408.
70) Genevay S, Finckh A, Payer M, et al. Elevated levels of tumor necrosis factor-alpha in periradicular fat tissue in patients with radiculopathy from herniated disc. Spine 2008; 33:2041-2046.
71) Mulleman D, Mannou S, Griffoul I, et al. Pathophysiology of disc-related sciatica. Evidence supporting a chemical component. Joint Bone Spine 2006;73:151-158.
73) Jacobs WCH, van Tulder M, Arts M, et al. Surgery versus conservative management of sciatica due to a lumbar herniated disc: a systematic review.
74) Weber H. 1982 Volvo Award in Clinical Science. Lumbar disc herniation: a controlled, prospective study with ten years of observation. Spine 1982;8:131-140.
75) Albert HB, Briggs AM, Kent P, et al. The prevalence of MRI-defined spinal pathoanatomies and their association with Modic changes in individual seeking care for low back pain. Eur Spine J 2011;20:1355-1362.
76) Shamji MF, Setton LA, Jarvis W, et al. Proinflammatory cytokine expression profile in degenerated and herniated human intervertebral disc tissue. Arthritis Rheum2010; 62:1974-1, 982.
77) Geiss A, Larsson K, Rydevik B, et al. Autoimmune properties of nucleus pulposus: an experimental study intakes. Spine 2007;32:168-173.
78) Marshall LL, et al. Chemical radiculitis: a clinical, physiological, and immunological study. Clin Orthop 1977; 129:61-67.
79) Takahashi N, Yabuki S, Aoki Y, Kikuchi S. Pathomechanisms of nerve root injury caused by disc herniation: an experimental study of mechanical compression and chemical irritation. Spine 2003; 28:435-441.
80) Smyth MJ, Wright V. Sciatica and the intervertebral disc: an experimental study. J Bone Joint Surg Am 1958; 40-A: 1401-1418.
81) Jacobs WCH, van Tulder M, Arts M, et al. Surgery versus conservative management of sciatica due to a lumbar herniated disc: a systematic review. Eur Spine J 2011; 20:513-522.
82) McNally DS, Shackleford IM, Goodship AE, Mulholland RC. In vivo stress management can predict pain on discography. Spine 1996; 21:2580-2587.
83) Nygaard OP, Mellgren SI. The function fo sensory nerve fibers in lumbar radiculopathy. Spine 1998;23:348-353.
84) Garfin SR, Rydevik B, Lind B, Massie J. Spinal nerve root compression. Spine 1995; 20:1810-1820.
85) Byrod G, Olmarker K, Konno S, et al. A rapid transport route between the epidural space and the intraneural capillaries of the nerve roots. Spine 1995; 20:138-143.
86) Lindblom K, et al. Spinal nerve injury in dorsolateral protrusions of lumbar discs. J Neurosurg 1948;5:413-432.
87) Lindahl O, et al. Histological changes in spinal nerve roots of operated cases of sciatica. Acta Orthop Scand 1951; 20:215-225.
88) Olmarker K, Rydevik B, Nordborg C. Autologous Nucleus pulposus induces neurophysiologic and histologic change in porcine cauda equina nerve roots. Spine 1993; 11:1425-1432.
89) Rydevik B, Brown MD, Lundborg G. Pathoanatomy and pathophysiology of nerve root compression. Spine 1984;9:7-15.
90) Takahashi K, et al. Nerve root pressure in lumbar disc herniation. Spine 2003; 21, October 1999?
91) Gertzbein SD, et al. Auto-immunity in degenerative disc disease of the lumbar spine. Ortho Clin North Am 1975; 6:67-73.
92) Mundt DJ, et al. An epidemiologic study of non-occupational lifting as a risk factor for herniated lumbar intervertebral disc. The Northeast collaborative group on low back pain. Spine 1993;18:595-602.
93) Sorensen IG, Jacobsen P, Gyntelberg F, et al. Occupational and other predictors of herniated lumbar disc disease – a 33 year follow-up in the Copenhagen mail study. Spine 2011; 36:1541-1546.
94) Harrington JF, Sungarian A, Rogg J, et al. The relationship between vertebral endplate shape and lumbar disc herniations. Spine 2001; 26:2133-2138.
95) Jarvik JG, Hollingworth W, Heagerty PJ, et al. Three-year incidence of low back pain in an initially asymptomatic cohort: clinical and imaging risk factors. Spine 2005;30:1541-1548.
96) Kobayashi S, Kokubo Y, Uchida K, et al. Effect of lumbar nerve root compression I'm primary sensory neurons and their central branches: changes and nociceptive neuropeptides substance P and somatostatin. Spine 2005;30:276-282.
97) Stadnik TW, et al. Annular tears and disc herniation: prevalence and contrast enhancement on MR images in the absence of low back pain or sciatica. Radiology 1998; 206:49-55.
98) Bendix T. (2004) Disc Herniation: Definitions and Types. In Herkowitz HN, Dvorak J, Bell G, et al. (Ed.), The Lumbar Spine (pp. 399-406). Philadelphia, PA: Lippincott, Williams, & Wilkins.
99) Toyone T, Tanaka T, et al. 'Low-back pain following surgery for lumbar disc herniation. A prospective study.' J Bone Joint Surg Am. 2004 May;86-A(5):893-6 "Excision of a herniated disc for relief of sciatica provided rapid relief of sciatica and low-back pain. The findings of the present small study suggest that ."
100) Deyo RA, Weinstein JN. Low back pain. N Engl J Med
101) Weinstein JN, et al. "Surgical vs nonoperative treatment for lumbar disc herniation: The Spine Patient Outcomes Research Trial (SPORT): A randomized trial. JAMA 2006; 296:2441-2450
103) Gibson JNA, Waddell G. “surgical interventions of lumbar disc prolapse." Cochrane Database Syst Rev 2009; (1): CD001350.
104) Osborn AG. "Nonneoplastic disorders of the spine and spinal cord." In :Diagnostic neuroradiology. St Louis, Mo: Mosby, 1994; 820-875.
105) Bruske-Hohlfeld I, Merritt JL, Onofrio BM, et al. Incidence of lumbar disc surgery: A population-based study in Olmsted County, Minnesota 1950-1979.
106) Peul WC, van Houwelingen HC, van den Hout WB, et al. Surgery versus prolonged to conservative treatment for sciatica. N Engl J Med 2007;356:2245-2256.
107) el Barzouhi A, et al. Influence of low back pain and prognostic value of MRI in sciatica patients in relation to back pain. PloS One 2014; 9:e90800.
108) Lequin MB Verbaan D, Jacobs WCH, et al. surgery versus prolonged conservative treatment for sciatica: five-year results of a randomized control trial. BMJ Open 2013;3:e002534.
109) Parr AT, Diwan S, Abdi S. Lumbar interlaminar epidural injections in managing chronic low back pain and lower extremity pain: a systematic review. Pain Physician 2009;12:163-188.
110) Chou R, Atlas SJ, Stanos SP, Rosenquist RW. Nonsurgical interventional therapies for low back pain: a review of the evidence for an American Pain Society clinical practice guideline. Spine 2009;34:1078-1093.
111) Wood KB, Fritzell P, Dettori JR, et al. Effectiveness of spinal fusion versus structured rehabilitation in chronic low back pain patients with and without isthmic spondylolisthesis. A systematic review. Spine 2011; 36:S110-S119.
112) Vroomen P, et al. Conservative treatment of sciatica: a systematic review. J Spinal Disord 2000; 13:463-469.
113) Arden NK, et al. A multicenter randomized control trial of epidural corticosteroid injections for sciatica. Rheumatology 2005; 44:1399-1406.
117) Boswell MV, Singh V, Manchikanti L, et al. "Interventional techniques: Evidence-based practice guidelines in the management of chronic spinal pain." Pain Physician 2007; 10:7-111.
118) Manchikanti L, et al. " Physician payment 2008 for interventionalists: current state of health care policy." Pain Physician 2007; 10:607-626.
119) Manchikanti L, Singh V, Hirsch JA, et al. "Analysis of growth in interventional techniques in managing chronic pain in Medicare population: a 10-year evaluation from 1997 to 2006. Pain Physician 2009; 12:9-34.
120) Kapural L, Vrooman B, Sarwar S, et al. A randomized, placebo-controlled trial of transdiscal radiofrequency biacuplasty for treatment of discogenic low back pain. Pain Med 2013; 14:362-373.
121) Simmonds MC, Brown JVE, Heirs MK, et al. Safety and effectiveness of recombinant human bone morphogenetic protein-2 for spinal fusion; a meta-analysis of individual-participant data. Ann Intern Med. 2013;158:877-889.
122) Fu R, Selph S, McDonagh M, et al. Effectiveness and harms of recombinant human bone morphogenetic protein-2 in spine fusion. A systematic review and meta-analysis. Ann Intern Med 2013;158:890-902.
123) Fetzer A, Scott DR. Nonsurgical treatment of herniated nucleus pulposus. In: Phillips FM, Lauryssen C, eds. The lumbar intervertebral disc. New York, NY: Thieme; 2010:86-91.
124) Karaman H, Kavak GO, Tufek A, et al. The complications of transforaminal lumbar epidural steroid injections. Spine 2011; 36:E819-E824.
125) Vad VB, Bhat AL, Lutz GE, et al. Transforaminal epidural steroid injections in lumbosacral radiculopathy: a prospective randomized study. Spine 2002; 27:11-16.
126) Saal JA, Saal JS. Nonoperative treatment of herniated lumbar intervertebral disc with radiculopathy: an outcome study. Spine 1989;14:431-437.
127) Weinstein SM, Herring SA, Derby R. Contemporary concepts in spine care: epidural steroid injections. Spine 1995; 20:184-186.
128) Lutz GE, et al. Fluoroscopic transforaminal lumbar epidural steroids: an outcome study. Arch Phys Med Rehab 1998; 79:1362-1366.
130) Manchikanti L, Cash KA, McManus CD, et al. A randomized, double-blind, active-controlled trial of fluoroscopic lumbar interlaminar epidural steroid injections in chronic axial or discogenic low back pain: results of two-year follow-up. Pain Physician to 13;16:E491-E504.
131) Rados I, Sakic K, Fingler M, et al. Efficacy of interlaminar versus transforaminal epidural steroid injection for the treatment of chronic unilateral radicular pain: prospective randomized study. Pain Medicine 2011; 12:1316-1321.
132) Parr AT, et al. Caudal epidural injections in the management of chronic low back pain: a systematic appraisal of the literature. Pain Physician 2012;15:E159-198.
133) Maigne JY, Rime B, Delignet B. Computed tomographic follow-up of 48 cases of nonoperatively treated lumbar intervertebral disc herniation. Spine 1992; 17:1071-1074.
134) Ikeda T, et al. Pathomechanism of spontaneous regression of the herniated lumbar disc: histologic and immunohistochemical study. J Spinal Disord 1996;9:136-140.
135) Ahn SH, Ahn MW, Byun WM. Effect of transligamentous extension of lumbar disc herniations and their regression in the clinical outcome of sciatica. Spine 2000; 25:475-480.
136) Komori H, Shinomiya K, Nakai O, et al. The natural history of herniated nucleus pulposus with radiculopathy. Spine 1996; 21:225-229.
137) Saal JA, Saal JS, Herzog RJ. The natural history of lumbar intervertebral disc extrusions treated non-operatively. Spine 1990;15:683-686.
138) Machi M, et al. Spontaneous regression of sequestered lumbar disc herniations: literature review. Clin Neurol Neurosurg 2014;120C:136-141.
139) Ito T, Yamada M, Ikuta F, et al. Histologic evidence of absorption of sequestration-type herniated disc. Spine 1996; 21:230-234.
149) Manchikanti L, Derby R, Helm S, Hirsch JA, et al. “a systematic review of mechanical lumbar disc decompression with nucleoplasty." Pain physician That 2009; 12:561-572.
150) Singh VJ, et al. “Percutaneous disc decompression using Coblation (nucleoplasty) in the treatment of chronic discogenic pain." (2002) Pain Physician; 5(3): 250-59.
151) Derby R, et al. "evidence informed management of chronic low back pain with minimally invasive nuclear decompression." Spine J 2008; 8:150-151.
152) Nykvist F. et al. "Severe sciatica: a 13 year follow-up of 342 patients." Eur Spine J 1995;4:335-338.
153) Balague' F. Et al. "recovery of severe sciatica." Spine 1999; 24:2516-2524.
154) Fjeld O, et al. "Prognostic factors for persistent leg pain in patients hospitalized with acute sciatica." Spine 2017; 42:E272-E279.
125) Mixter WJ, Barr JS. “Rupture of the intervertebral disc with involvement of the spinal canal.” N Engl J Med 1934; 211:210-5
170) Karppinen J, et al. “Severity of Symptoms and Signs in Relation to Magnetic Resonance Imaging Findings Among Sciatic Patients.” Spine 2001; 26:E149-E154
290) Kortelainen P, et al. “Symptoms and signs of sciatic and their relation to the location of the lumbar disc herniation.” Spine – 1985; 10:88-92
Experiment: R5-v-R5M2--8000iso
{kind=link}
Top | Home